Download
1 / 36
360 likes | 555 Views
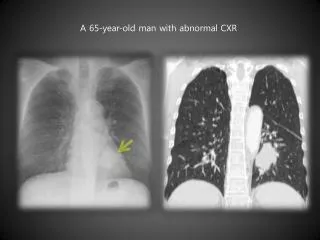
Lymphoma Education Day 13 th October 2010 The modern management of Hodgkin lymphoma John Radford Manchester Academic Health Science Centre Manchester, UK. CXR of 30 year old female before treatment. Before starting treatment.

E N D
Lymphoma Education Day13th October 2010The modern management of Hodgkin lymphomaJohn RadfordManchester Academic Health Science CentreManchester, UK
Before starting treatment • Biopsy of enlarged lymph node and central review by expert lymphoma pathologist • Investigations to determine stage; bloods, CT scan of thorax, abdomen, pelvis, PET scan, BM biopsy if not stage IA or IIA • Discussion with colleagues at MDT meeting • Discussion with patient; treatment options, relevant clinical trials, immediate and late side effects
Treatment for HL • Treatment for limited stage (IA and IIA): 3 cycles chemotherapy +/- RT; 90% cure • Treatment for advanced stage (II plus B symptoms or bulk and/or B symptoms, III and IV); 6 cycles chemotherapy +/- RT; 70% cure • Treatment for firstrecurrence; 2nd line chemotherapy followed by autologous or allogeneic transplantation • Treatment for subsequent recurrence; new drugs (panobinostat, iodine131 basiliximab, brentuximab vedotin) in clinical trial
ABVD (days 1 and 15 of a 28 day cycle) • Adriamycin; hair loss, nausea and vomiting, myelosuppression, cardiotoxicity • Bleomycin; shivers and shakes, skin pigmentation, pulmonary toxicity • Vinblastine; nausea, myelosuppression, neuropathy • Dacarbazine; nausea and vomiting, myelosuppression, painful veins during drug infusion
The early days: RT alone • Imaging limited to plain radiology of the thorax and lymphangiography of the abdomen and pelvis • These techniques had low sensitivity for upper abdominal and splenic disease • Staging laparotomy performed (splenectomy, liver and lymph node biopsies) to enhance sensitivity • If all tissues histologically negative, patient said to have pathological stage (PS) I/II and treated with “mantle field” RT
Extended field RT Rosenberg and Kaplan, 1970
Cures resulted, but… • Despite pathological staging, relapse occurred in ~30% mainly outside the radiation field • In addition, staging laparotomy associated with • immediate mortality and morbidity • delay to start of chemotherapy in those requiring it • greatly increased risk of fatal septic shock (Donaldson et al, NEJM, 1972)
Adjuvant MOPP/MVPP(Anderson et al, BJC) • 114 pts with PS IA-IIB HL randomised to receive either mantle RT alone or mantle RT followed by 6 cycles MVPP • After median follow-up of 62 mo • RFS was 69% for RT alone and 93% for RT+MVPP (p=0.0003) • Overall survival was 93% with no difference between trial arms (p= 0.54) because of successful salvage
Relapse free survival Overall survival Anderson et al, Br J Cancer 1984, 49, 695-702
The move towards smaller RT fields • GHSG HD8 trial involving 1204 pts with stages I-II and risk factors • Randomised between COPP/ABVD x 2 followed by either EFRT plus boost or IFRT plus boost (Engert et al 2003) • no difference in terms of CR, FFTF, OS • more toxicity with EFRT
…and smaller RT doses • GHSG HD1 trial (Diehl et al, 1995) • stages I and II with unfavourable features • COPP/ABVD x 2 (total of 4 cycles chemo) followed by either 20Gy or 40Gy of EFRT to non-bulky sites (40 Gy to bulk) • GHSG HD5 trial (Loeffler et al, 1997) • similar group of patients • same chemo followed by 30Gy of EFRT to non-bulky areas (40 Gy to bulk) • concluded that no relevant RT dose effect exists in the range 20-40 Gy and doses of 20 Gy sufficient for non-bulky sites (40 Gy to bulk) after 4 cycles of modern chemo
Chemotherapy alone? • NCI Canada and ECOG: 399 patients stratified as unfavourable (any of age ≥40, ESR ≥50, MC or LD histology, ≥4 sites of disease) or favourable (none of the above) (Meyer et al, 2005) • Randomised to a treatment that included RT (STLI for favourable or ABVD x 2 plus STLI for unfavourable) or no RT (ABVD x 4-6 depending on response) • FFP at 5 years superior in RT group (93% vs 87%) due to reduced levels of disease control in unfavourable group receiving ABVD alone • no difference in OS due to better FFP offset by deaths from causes other than HL
Results encouraging but caution necessary • EORTC/GELA H9-F trial (Eghbali et al, 2005) in favourable patients in CR after EBVP x 6 (epirubicin, bleomycin, vinblastine, prednisolone) randomised to receive either: • IFRT 36 Gy • IFRT 20Gy • No RT • Trial halted in line with early stopping rules
Q: Can PET identify those patients who need RT after CT and those who do not?
Q: Can PET identify those patients who need RT after CT and those who do not? A: It’s an attractive idea but the case is not yet proven
“Negative” PET scan after treatment (no disease identified)
UK NCRI RAPID trial Initial treatment: ABVD x 3 Re-assessment: if NR/PD, patient goes off study if CR/PR, FDG-PET scan performed PET +ve PET -ve 4th cycle ABVD then IFRT Randomisation IFRT No further treatment
Status at 2nd interim analysis (presented ASH 12/08) 369 patients registered; 190 male, 179 female, median age 34.5 years 331 have had a PET scan after 3 cycles ABVD Score 1, 203 (61%) Score 2, 58 (18%) Score 3, 35 (11%) Score 4, 20 (6%) Score 5, 15 (4%) Score 1,2 -ve (261, 79%); score3,4,5 +ve (70, 21%)
Status - 2 257 of 261 PET -ve pts have been randomised Involved field RT (n=125, 49%) No further treatment (n=130, 51%) Outcome of randomisation entered after database locked for analysis (n=2) 4 pts not randomised Patient choice (n=2) Clinician choice (n=1) Error (n=1)
Status - 3 Median follow-up of 13 mo from randomisation 245 of 255 (96%) pts are alive and progression-free 6 (2%) have progressed 4 (1.5%) have died (HL 1, treatment related 1, other 2)
0.20 Hodgkin lymphoma (60 deaths) Second malignancy (59 deaths) Cardiopulmonary (22 deaths) 0.15 Other (13 deaths) Infection (7 deaths) Probability 0.10 0.05 0.0 0 5 10 15 20 25 30 Years Causes of death in patients aged < 50 (P Mauch, Bellagio, July 2004)
Breast cancer screening in the UK • Recommended for women receiving RT to the chest below age 36 and… • Now aged ≥25 and ≥8 years since treatment • Annual MRI/ultrasound ages 25-30 • Annual mammography ages 30 and over until age 50 (then every 3 years)
Screening for lung cancer • By the time symptoms have developed the prognosis is often poor • Long latency following treatment so opportunities for screening in this very high risk population • Exploratory screening study (HOLYSTIC) has been proposed and this to be discussed at forthcoming international meeting in Cologne
Cardiovascular disease • Increased risk of heart failure, fatal infarction (2.5 x background risk, Swerdlow et al, JNCI 2007) and stroke following doxorubicin containing CT and RT • Before treatment; assess heart function in the older patient and those with a history • After treatment; screen for high BP, lipids and diabetes mellitus
Conclusions - 1 • Pathological staging in HL is unnecessary • Smaller fields of RT are as effective as larger fields and a dose of 20Gy is sufficient for non-bulky sites • CT plus RT is superior to RT alone and in terms of choice of CT regimen, ABVD is the current standard of care
Conclusions - 2 • Risk adapted therapy making use of pre-treatment factors is entirely valid • Response adapted therapy using FDG-PET to determine the need for consolidation RT after CT is under investigation • Allogeneic transplantation and new agents are under investigation
Conclusions - 3 • In the long term the greatest threat to Hodgkin survivors is from the late effects of treatment • Breast cancer screening guidelines have existed in the UK since 2004 but need to be better implemented • Screening for lung cancer is under investigation • Cardiovascular morbidity/mortality remains a major challenge and requires a multi-disciplinary research effort
Finally • Evolution of treatment for Hodgkin lymphoma is a success story spanning 5 decades • Significant challenges remain • So all patients should be offered the opportunity to take part in relevant clinical trials at presentation and at relapse • Unless this happens, treatment gets stuck and progress will grind to a halt