Download
1 / 38
380 likes | 497 Views
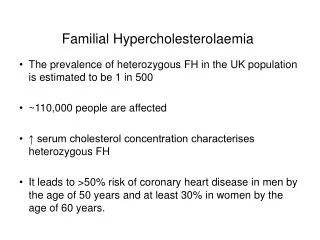
FAMILIAL CLL Ashkelon – 2006 Daniel Catovsky. 1887 +1953. 1884 +1996. 1894 +1968. 1895 +1984. 1897 +1928. 1900 +1980. 1903 +1968. CLL. 1907. 1909. 1912 +1912. 1915. 1917 +1980. 1925. 1919 +1994. Familial risks of CLL. The main evidence derives from:

E N D
FAMILIAL CLL Ashkelon – 2006 Daniel Catovsky
1887 +1953 1884 +1996 1894 +1968 1895 +1984 1897 +1928 1900 +1980 1903 +1968 CLL 1907 1909 1912 +1912 1915 1917 +1980 1925 1919 +1994
Familial risks of CLL The main evidence derives from: Cohort studies – risk 2.4-5.7(Gunz, 1975; Giles, 1984; Goldgar, 1994) Case control studies – risk 2.3-4.3(Linet, 1989; Pattern, 1991; Cartwright, 1987) Relatives of CLL patients have a six-fold increase in risk
Familial risks of B-cell LPDs Evidence of pleiotropism Goldin et al., (2004) Blood 104:1850; Goldin et al., (2004) Cancer100; 1902 Goldin et al., (2004) Cancer Epid Bio Prev 13:1415
Monoclonal B-cell lymphocytosis (MBL) • Diagnostic criteria recently reported • (Marti et al, BJH 130:325, 2005) • Flow cytometry can detect ‘sub-clinical’ MBL in normal relatives of F-CLL and provides the possibility of extending the number of affecteds in linkage families • MBL is found in 3.5% of normal adults by flow cytometry • (Rawstron et al, Blood 100:2289 & 100:635, 2002)
CD5 Familial Control CD79b CD20 Incidence of MBL in Familial CLL Rawstrom et al (2002) 25% 20% 15% 10% 5% 0% years <50 50-59 60-69 70+
MBL in F-CLL: young adults show the highest relative risk* *Tute, Yuille, Rawstron et al (2006) Leukemia 20:728
The relationship between • MBL and CLL* • Cluster analysis with 18 antigens showed that MBL and CLL cases clustered together, separate from normal B-cells • Purified MBL B-cells showed: • 13q14 del in 16/35 cases • Trisomy 12 in 3/21 cases • Clonal homogeneity in 5/12 • VH gene family usage as CLL * Presented in IWCLL (2005) by Bennett, Hillmen, Rawstron et al
UK Familial CLL study • Families collected to date • 456 families documented (339 with 2 or more CLL cases) • 401 of these we have at least 1 sample from the family • 87 families have at least 1 case of CLL and 1 or more cases of LPD • 33 families with 2 or more NHL/HL cases
UK Familial CLL study • Contributing countries • Over 250 UK families • 112 from Europe (incl. 58 Italy, 26 Spain & Portugal) • 33 Australia & New Zealand • 12 USA & Canada (mostly self-referrals) • 14 Middle-Eastern (mainly Israel)
Family 005 Family 094 Family 037 Family 039
Videbaek’s pedigree 14 revisited (1947-2004)* Original family = 55 members Current pedigree = 221 descendents 10 diagnosed with CLL; 1 T-cell lymphoma 18 non-haematological cancers (5 breast) Relative risk for B-cell LPD = 7.9 (p < 0.001) This family provides further support for an inherited predisposition to CLL *Jønsson, Houlston, Catovsky et al (Leukemia, 19, 1025, 2005)
Anticipation in Familial CLL Yuille (1998) Goldin (1999) Wiernik (2001) # families 10 13 10 Mean age 74 68 72 Mean age 52 51 51 A large epidemiological study showed no evidence of anticipation in CLL & NHL: Daugherty et al ,Cancer Epidemiol Biomarkers Prev.(2005) 14:1245
Familial CLL No differences from sporadic CLL in: • Age, M:F ratio, incidence of Zap-70+ * • IgVH usage and frequency of somatic mutation * • ATM mutations • Frequency of 6q21, 11q23, 13q14 and p53 deletions or trisomy 12 * Rassenti et al (2003) Blood 102:670a A study from the USA CLL Research Consortium
Strategies for identifying CLL predisposition genes • 1: Linkage analysis of families to identify moderate-high penetrance alleles • 2: Association studies of SNPs to identify low penetrance alleles • 3: Screening familial cases for mutations in candidate genes
CLL linkage analysis: method • Examines regions of haplotype sharing in the DNA of affected individuals within each family • This determines the areas which deviate from the expected normal ratios 25 : 50 : 25 across the genome • A positive linkage score is established if affecteds share 1 or 2 alleles more than expected in a given region
CLL linkage analysis: method • Analysis of families segregating CLL/B-Cell LPDs using DNA polymorphisms • 2 types of DNA polymorphisms can be used: • microsatellites (simple repeats eg. CACACACA) • SNPs (eg. C/T) • Until recently microsatellites were the most popular marker of choice for whole genome scans in order to identify predisposition loci
Linkage analysis in Familial CLL • One previous whole genome linkage search, undertaken in 18 CLL families studied using microsatellites, was extended recently to 28 (16 families were the same in both) • No regions were identified that attained statistical significance in these studies focusing on chromosomes 1, 3, 6, 12, 13 and 17 • Chromosome 13q21-q23 remains of interest but was not statistically significant for linkage in the context of a whole genome scan Goldin et al., Br J Haem 121:866 (2003); Ng et al Br J Haem 133:59 (2006)
Linkage analysis in Familial CLL A high density single nucleotide polymorphism (SNP) - based genomewide linkage search was undertaken on 115 CLL families by our group using the Affymetrix Mapping 10K Array (11,555 markers)
Comparison of Affymetrix 10K SNP array marker coverage to 400 ABI marker microsatellite panel SNPsMicrosatellites The SNP array offers greater density of markers with the flexibility of adding more samples at any time in the analysis as they are recruited
Linkage analysis in Familial CLL • Sample set used for SNP linkage analysis: • 115 CLL/CLL-LPD families • 80 families with 2 affecteds • 28 families with 3 affecteds • 5 families with 4 affecteds • 2 families with 5+ affecteds • Median age at diagnosis of CLL 61 years Sellick et al, Am J Hum Genetics (2005) 77:420-9
Plots of linkage statistics after the removal of high-LD SNPs* *Sellick et al, Am J Hum Genet, 77: 420 (2005)
Familial CLL – linkage analysis Sellick et al, Am J Hum Genet, 77, 420 (2005)
Linkage analysis: future work • Genotyping an additional 40 families • Screening family members for MBL status • Currently undertaking mutation screening of genes mapping to linked regions e.g. the 11p11 locus: SPI1 and MADD
Strategies for identifying CLL predisposition genes • 1: Linkage analysis of families to identify moderate-high penetrance alleles • 2: Association studies of SNPs to identify low penetrance alleles • 3: Screening familial cases for mutations in candidate genes
Genetic association studies • Part of the susceptibility to B-cell LPDs is likely to be polygenic • The identification of low penetrance alleles are contingent on association studies with significant statistical power
Genetic association studies An issue of power Houlston & Peto, Human Genetics112: 434 (2003)
Genetic association studies No genetic linkage or allelic association detected with: • Dok1 gene (2p13) • P2X7 gene polymorphisms (12q24) • MTHF gene polymorphisms (1p36) • ARLTS1 coding SNPs (13q14) • proposed by Calin et al N Eng J Med 352:1667 (2005)
Germline variants of ARLTS1 and risk of F-CLL • ARLTS1 is a putative tumour-suppressor gene, a member of the RAS superfamily at 13q14, a region commonly deleted in CLL • Calin et al (2005) proposed that a truncating sequence change in ARLTS1, G446A (Trp149Stop), predisposes to CLL and other malignancies based on findings in 17 familial CLL cases of mixed ethnicity
Germline variants of ARLTS1 and risk of CLL* • We conducted an association study to determine if the proposed variant, or 5 other coding SNPs in ARLTS1,predispose to CLL • We studied germline DNA from 413 CLLs (all British Caucasians) and 471 matched controls by direct sequencing * Sellick et al, NEJM 2006: letter & Leukemia Research, 2006 (in press)
Germline variants of ARLTS1 and risk of CLL* • All 6 ARLTS1 SNPs were polymorphic in patients and controls with no evidence of population stratification • No association was found between any of the 6 cSNPs and risk of CLL • In addition, no evidence for an association between ARLTS1 haplotypes and risk of CLL nor with familial CLL (158 cases of F-CLL included) was identified * Sellick et al, NEJM 2006: letter & Leukemic Research, 2006 (in press)
Pathogenesis of Familial CLL • High-penetrance mutations • [Genome-wide linkage analysis] • OR • Polygenic model of low penetrance alleles • [Association studies in ethnically matched cases and controls comparing the frequency of polymorphic genotypes]
Pathogenesis of CLL • New association study • We adopted a candidate gene-based approach through an association study evaluating cSNPs from genes likely to be involved in cancer • We genotyped coding non-synonymous SNPs that alter the amino acid sequence • greater likelihood of influencing gene function and/or expression
Variants in the ATM-BRCA2-CHEK2 axis confer susceptibility to CLL* • Large scale association study in UK Caucasians to identify low penetrance susceptibility alleles for CLL: we tested 992 CLLs and 2707 controls • To increase the likelihood of identifying disease-causing alleles we genotyped a set of 1467 non-synonymous SNPs from 865 candidate cancer genes using Illumina Arrays * Rudd, Sellick et al, Blood, 2006 (in press)
Variants in the ATM-BRCA2-CHEK2 axis confer susceptibility to CLL* • Significant associations were identified in SNPs mapping to 9 genes pivotal to DNA damage-response and cell-cycle pathways including: • ATM, BRCA2, CHEK2, BUB1B, EGF & MMP9 • Main associations were seen between risk of CLL and minor alleles of ATM, CHEK2, BRCA2 & BUB1B strongly suggesting that variants in the DNA damage-response axis are implicated in predisposition to CLL * Rudd, Sellick et al, Blood, 2006 (in press)
Rudd et al, Blood 2006 (in press) Inter-relationship between genes involved in the DNA damage-response axis for which cSNPs were associated with risk of CLL
UK Familial CLL study • Top collaborators worldwide • UK: RMH/ICR - 59 families • Prof Dyer – 14 • Italy: Dr Mauro – 30 • Dr Capalbo – 6 • Australia: Prof Wiley – 11 • Drs Westerman/Seymour - 5 • Norway/Denmark: Prof Jønsson - 11 • Portugal: Dr Ribeiro - 7 • Israel: Drs Berrebi/Stark - 5
Work supported by: ARBIB FOUNDATION ICR Section of Cancer Genetics Prof Richard Houlston (team leader) Dr Gabrielle Sellick (principal investigator) Dr Ruwani Gunaratne (data manager)