Download
1 / 36

E N D
Acute colonic ischaemia:The splenic flexure and descending colon have little collateral circulation and lie in ‘watershed’ areas of arterial supply. The spectrum of injury ranges from reversible colopathy to transient colitis, colonic stricture, gangrene and fulminant pancolitis. Arterial thromboembolism is usually responsible but colonic ischaemia can also follow severe hypotension, colonic volvulus, strangulated hernia, systemic vasculitis or hypercoagulable states. Ischaemia of the descending and sigmoid colon is also a complication of abdominal aortic aneurysm surgery (where the inferior mesenteric artery is ligated).The patient is usually elderly and presents with sudden onset of cramping, left-sided, lower abdominal pain and rectal bleeding.
Symptoms usually resolve spontaneously over 24–48 hours and healing occurs in 2 weeks.Some may develop a fibrous stricture or segment ofcolitis. A minority develop gangrene and peritonitis.The diagnosis is established by colonoscopy within 48 hours of presentation; otherwise, mucosal ulceration may have resolved. Resection is required for peritonitis.
Chronic mesenteric ischaemia:This results from atherosclerotic stenosis of the coeliac axis, superior mesenteric artery and inferior mesenteric artery. At least two of the three vessels must be affected for symptoms to develop. The typical presentation is with dull but severe mid- or upper abdominal pain developing about 30 minutes after eating. Weight loss is common because the patient is reluctant to eat, and some experience diarrhoea. Physical examination shows evidence of generalised arterial disease. An abdominal bruit is sometimes audible but is non-specific.The diagnosis is made by mesenteric angiography.Treatmentis by vascular reconstruction or percutaneous angioplasty, if the patient’s clinical condition permits. The condition is frequently complicated by intestinal infarction, if left untreated.
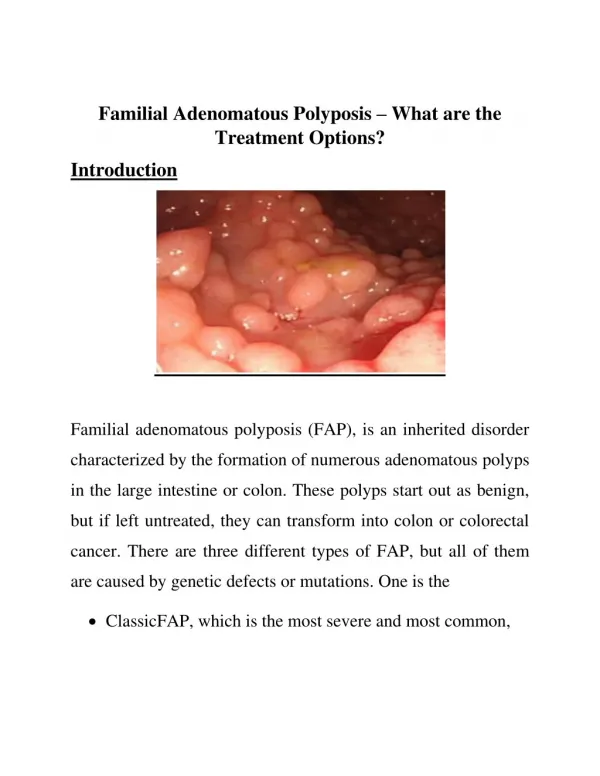
Familial adenomatous polyposis (FAP) is an uncommonautosomal dominant disorder affecting 1 in 13 000 of the population and accounting for 1% of all colorectalcancers. It results from germline mutation of the tumoursuppressor APC gene, followed by acquired mutation ofthe remaining allele.Around 20% of cases arise as new mutations andhave no family history. Hundreds to thousands ofadenomatous colonic polyps develop in 80% of patientsby age 15 , with symptoms such as rectal bleeding beginning a few years later.
In those affected, cancer will develop within 10–15 years of the appearance of adenomas and 90% of patients will develop colorectal cancer by the age of 50 years. Despite surveillance, approximately 1 in 4 patients with FAP havecancer by the time they undergo colectomy.Duodenal adenomas occur in over 90% and aremost common around the ampulla of Vater , Malignant transformation to adenocarcinoma occurs in 10% and is the leading cause of death in those who have had prophylactic colectomy.
Familial adenomatous polyposis. There are hundreds of adenomatous polyps throughout the colon.
Early identification of affected individuals beforesymptoms develop is essential. The diagnosis can be excluded if sigmoidoscopy is normal. In newly diagnosed cases, genetic testing should be carried out to confirm the diagnosis and identify the causal mutation.Subsequently, all first-degree relatives should also undergo testing.
In families with known FAP, family members should undergo mutation testing at 13–14 years of age and patients who are found to have the mutation should be offered colectomy after school or college education has been completed. The operation of choice is total proctocolectomy with ileal pouch–anal anastomosis. Periodic upper gastrointestinal endoscopy every 1–3 years is recommended.
Peutz–JegherssyndromeMultiple hamartomatous polyps occur in the small intestine and colon, as well as melanin pigmentation of the lips, mouth and digits . Most cases are asymptomatic, although chronic bleeding, anaemia or intussusception can occur. There is a significant risk of small bowel or colonic adenocarcinoma and of cancer of the pancreas, lung, ovary, breast and endometrium. It is an autosomal dominantly inherited disorder, most commonly resulting from truncating mutations in a serine– threonine kinase gene on chromosome 19p (STK11).
Diagnosisrequires two of the three following features:• small bowel polyposis• mucocutaneous pigmentation• a family history suggesting autosomal dominant inheritance.The diagnosis can be made by genetic testing but this may be inconclusive, since mutations in genes other thanSTK11 can cause the disorder. Affected people should undergo regular upper endoscopy, colonoscopy, and small bowel and pancreatic imaging.Polyps greater than 1 cm in size should be removed.
Testicular examination is essential for men, while women should undergo pelvic examination, cervical smears and regularmammography. Asymptomatic relatives of affected patients should also undergo screening.
Although relatively rare in the developing world, colorectal cancer is the second most common internal malignancy and the second leading cause of cancer deaths in Western countries. In the UK the incidence is 50-60 per 100 000, equating to 30 000 cases per year. The condition becomes increasingly common over the age of 50 years.
Pathophysiology:Both environmental and genetic factors are important incolorectal carcinogenesis .Environmental factorsaccount for 70% of all ‘sporadic’ colorectal cancers. Dietary factors are most important environmental factor.
Genetic Factors:Colorectal cancer development results from the accumulation of multiple genetic mutations arising from two major pathways: chromosomal instability and microsatellite instability.*Chromosomal instability: Mutations or deletions of portions of chromosomes arise, with loss ofheterozygosity (LOH) and inactivation of specifictumour suppressor genes.
*Microsatellite instability: This involves germlinemutations in one of six genes encoding enzymesinvolved in repairing errors that occur normallyduring DNA replication (DNA mismatch repair).A few sporadic cancers develop this way, as do most cases of hereditary non-polyposis colon cancer (HNPCC).
Hereditary Non-Polyposis Colon Cancer:(HNPCC) accounts for 5-10% of cancers; it occurs in those with a family history and often at a young age. this disorder have an autosomal dominant mode of inheritance. The lifetime risk of colorectal cancer in affected individuals is 80%. The mean age of cancer development is 45 years, and in contrast to sporadic colon cancer two-thirds of tumours occur proximally. In a subset of patients, there is also an increased incidence of cancers of the endometrium, ovary, urinary tract, stomach, pancreas, small intestine and central nervous system.
Those who fulfil the criteria for diagnosis should be referred for assessment, genetic testing and colonoscopy. These should begin around 25 years of age or 5-10 years earlier than the youngest case of cancer in the family. Colonoscopy needs to be repeated every 1-2 years, but even then, interval cancers can still occur.
Clinical features:Symptoms vary depending on the site of the carcinoma. *In tumours of the left colon, fresh rectal bleeding is common and obstruction occurs early.*Tumours of the right colon present with anaemia from occult bleeding or with altered bowel habit, but obstruction is a late feature.*Colicky lower abdominal pain is present in two-thirds of patients and rectal bleeding occurs in 50%. *Carcinoma of the rectum usually causes early bleeding, mucus discharge or a feeling of incomplete emptying.
Between (10 and 20)% of patients present with iron deficiency anaemia or weight loss.On examination there may be a palpable mass, signs of anaemia or hepatomegaly from metastases. Low rectal tumours may be palpable on digital examination.
Investigations:Colonoscopyis the investigation of choice because it is more sensitive and specific than barium enema. Furthermore, lesions can be biopsied and polyps removed. CT colonography ('virtual colonoscopy') is a sensitive non-invasive technique for diagnosing tumours and polyps greater than 1 cm that can be used if colonoscopy is incomplete or high-risk. CT is valuable for detecting hepatic metastases, although intraoperative ultrasound is increasingly being used for this purpose. The most accurate procedure for locoregional staging for rectal cancer is endoscopic ultrasonography.
A proportion of patients have raised serum carcinoembryonicantigen (CEA) concentrations but this is variable and so of little use in diagnosis. Measurements of CEA are valuable, however, during follow-up and can help to detect early recurrence.
Prevention and screeningFecal Occult Blood Test:*The test is inexpensive, noninvasive, generally acceptable to patients, and can detect bleeding anywhere in the colon. Two separate samples from each of three spontaneously passed stools (six samples) sould be taken. Patients should avoid ingesting aspirin, nonsteroidal anti-inflammatory drugs, vitamin C, and red meat for 2 days before the test. *Fecal occult blood testing is a poor test to detect polyps, which usually do not bleed and are associated with a large number of false-positive results that require further evaluation. *Decrease morality by 15-33%
Flexible sigmoidoscopy *It examine the colon from the rectum to the splenic flexure. *Flexible sigmoidoscopy with removal of any lesions is associated with a 60% to 70% reduction in mortality rates from colorectal cancer.*It easier to perform than colonoscopy.*Limitations of flexible sigmoidoscopy are that the proximal colonnot visualized. *Adding fecal occult blood testing to screening flexible sigmoidoscopy probably does not improve efficacy.
ColonoscopyColonoscopyevaluates the entire colon and can detect 95% of polyps ≥10 mm in diameter. Approximately 25% of adenomas identified by colonoscopy are in the proximal colon and beyond the reach of the flexible sigmoidoscope. Colonoscopy detects colorectal cancer in approximately 1% of asymptomatic persons undergoing screening, and any polyps found during this procedure can be removed for histologic examination. Disadvantages of colonoscopy include the cost and risk, as the rate of major complications (bleeding or perforation) is 1/1000 procedures. Patients are usually sedated and have to undergo a cleansing bowel preparation.
CT ColonographySensitivity for polyp detection by CT colonography is extremely variable. The sensitivity of CT colonography for polyps <5 mm varies from 30% to 60% whereas the range for lesions ≥1 cm is 60% to 95%. These data reflect variation in technique, scanner technology, and operators and readers. Concerns unique to CT colonography include radiation exposure, the relevance of small lesions, surveillance intervals, and how to address incidental findings. The radiation exposure of a single examination is low; however, such exposure would result in a radiation-induced tumor in 1 in 714 persons.
Fecal DNA TestingExfoliation of DNA is a constant event within the colon. This DNA can be recovered from the stool and analyzed for a panel of molecular aberrations linked with colorectal neoplasia.
ManagementSurgeryThose with locally advanced rectal cancer should be offered neoadjuvant radiotherapy or chemoradiotherapy to increase the subsequent chance of a complete surgical resection. A 1-week course of radiotherapy just prior to surgery reduces the risk of local recurrence in operable rectal cancer.
Adjuvant and palliative therapy:Adjuvant chemotherapy with 5-fluorouracil/folinicacid or capecitabine preferably in combination with oxaliplatin,these drugs also used as palliative chemotherapy.Patients with advanced metastatic disease may be treated with monoclonal antibodies using bevacizumab or cetuximab, either alone or together with chemotherapy.Pelvic radiotherapy is sometimes useful for distressing rectal symptoms such as pain, bleeding or severe tenesmus. Endoscopic laser therapy or insertion of an expandable metal stent can be used to relieve obstruction.