Download

1 / 39
390 likes | 521 Views
The State of Our Professions in Light of Health Care Change. Florence Clark, Ph.D., OTR/L, FAOTA AOTA President June 21, 2012. Components of My Talk. Major Changes to Health Care Policy. 2010-2020: The Decade of Health Care Reform.

E N D
The State of Our Professions in Light of Health Care Change Florence Clark, Ph.D., OTR/L, FAOTA AOTA President June 21, 2012
2010-2020:The Decade of Health Care Reform • Significant changes in the way the federal government supports health care • Increased regulation and accountability
2010-2013: Regulation and Coverage • Dependent coverage through age 26 • Elimination of: • pre-existing condition exclusionsfor children • lifetime limits
2014: Major Expansion of Coverage • Employer penalties if no provision for health coverage • Health insurer industry fee • Medicaid expansion
2015-2020: Bending the Cost Curve • Medicaid penalty for not adopting Electronic Medical Record software • IPAB (Independent Payment Advisory Board) • Excise tax on high-cost health plans (Cadillac plans) • Reduced payment for hospital-acquired conditions • Individual mandate becomes effective
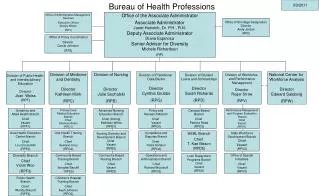
New Regulators • CMS Innovation Center • Reduces spending while increasing quality • Independent Payment Advisory Board (IPAB) • 15 members, make financial recommendations • Health Insurance Reform Implementation Fund • Implements policies • Patient-Centered Outcomes Research Institute (PCORI) • 36 member board, conducts research • National Prevention, Health Promotion, and Public Health Council • Funding for prevention and public health programs • U.S. Preventive Services Task Force (USPSTF) • Disseminate evidence on effective preventive services • Community-Based Collaborative Care Network (CCN) Program • Support and coordinate services for the underserved • Community Living Assistance Services and Supports (CLASS) • Provides in-home services to keep people out of long-term care facilities • Federal Coordinated Health Care Office (within CMS) • Coordinate Medicare and Medicaid • Workforce Advisory Committee • National workforce strategy
Old Model Linear
New Model Complicated Plan of Care
Paradigm Shifts in Primary Care Institute for Funcational Medicine: IFM White Paper: Jones et al (2010) 21st Century Medicine: A New Model for Medical Education and Practice
Emphasis on Collegiality and Teamwork http://www.toastmasters.org/MainMenuCategories/FreeResources/QuestionsaboutLeadership/Teamwork.aspx
Medicaid Population • New federal policies will increase national Medicaid enrollment by 40% by 2016 (~ 24 million more individuals) • Hospitals: • Learn to operate according to Medicaid rates • Aggressively market to the population
Fast Facts • 83% of health care expenditures in the U.S. are devoted to people with chronic conditions. • 3% of the population (those with 5 or more chronic conditions) consume 67% of health care resources. Source: Agency for Healthcare Research and Quality
Be Responsive to Trends • Social networking in health care • Web-based information • From sickness to wellness • Ramp up home/community-based health care • Home is where the innovation will happen • Nothing about us without us
Evidence-Based Practice Hoffman, T., Bennett, S. & DelMar, C. (2010). Introduction to evidence-based practice. In T. Hoffman, S. Bennett & C. DelMar (Eds.). Evidence-based practice across the health professions, pp. 1-15. Elsevier Australia: Chastswood, NSW. Evidence-based practice is “the integration of the best research evidence with clinical expertise and the client’s values and circumstances. It also requires the health professional to take into account characteristics of the practice contextin which they work.” (Hoffman, Bennett & DelMar, 2010, p. 3)
The healthcare practitioner’s tendency towards inquiry A Spanish study found improved persistence when an answer could be found in less than 2 minutes; whereas likelihood of continuing the search dropped to 40% if it took 30 mins or more Hoffmann, T., Bennett, S., Del Mar, C. (2010). Evidence-based practice: Across the health professions. Chatswood, New South Wales, Australia: Elsevier.
The Process of Evidence-based Practice:THE IDEAL Hoffman, T., Bennett, S. & DelMar, C. (2010). Introduction to evidence-based practice. In T. Hoffman, S. Bennett & C. DelMar (Eds.). Evidence-based practice across the health professions, pp. 1-15. Elsevier Australia: Chatswood, NSW.
The Process of Evidence-based Practice:THE REAL So what is the “Real World” Alternative? • Barriers: • Professional training • Time • Resources • Inclination to embrace EBP • Belief it is not needed • $ to afford workshops • Research not viewed as relevant to their practice
So How Can You Realistically Practice Using Evidence? Three Ways: Have a working knowledge of research designs and fluency in describing evidence Include evidence in your Mindlines Internalize a new identity as an evidence-based practitioner
Include evidence in your Mindlines Mindlines Clinician’s internalized guidelines for treatment based on: Educational foundations Clinical reasoning Experience Continually evolve with new information Gabbay, J. & Le May, A. (2011). Practice-based evidence for healthcare: Clinical mindlines. NY & London: Routledge.
Mindlines central guidance local guidance “they say” reps colleagues opinion leaders patients’ views experience journals and magazines infrastructure media teaching/training textbooks education sessions Gabbay, J. & Le May, A. (2011). Practice-based evidence for healthcare: Clinical mindlines. NY & London: Routledge. p. 46.
Patient-Centered Medicaid Medical Homes • Locally-based facilities • For patients with multiplechronic conditions • Care coordination • Multidisciplinary Team provides comprehensive care • Based on documented value of primary care
Accountability Care Centers (ACC) • Provider-led health care organization • Aligns primary & specialty services • Takes collective responsibility for improving patient care • Bundled care • Bonus on top of fee for service • Shared data • Payer retains risk • Law rewards improved outcomes • Increased alignment of services • Payer and provider are one partner (e.g. Kaiser) or share risk
Adherence & Quality • Increase patient adherence to therapy • Demonstrate impact of motivational, emotional, and contextual factors • Improve overall quality and outcomes • Think like consumers • Know community • Provide value
Research in Reform • $1.1 Billion has already been committed toward comparative effectiveness research • Evaluation of health care delivery methods: emphasis on prevention • A non-profit Patient Centered Outcomes Research Institute (PCORI) has been established
Innovation Established in the Health Care Reform Act • The Center for Medicare and Medicaid Innovation (CMI) to test innovative payment and delivery models that reduce cost and improve quality • Primary care payment reforms, including Patient Centered Medical Homes
Insurance Exchanges: 2014 • Statewide • Assure all services are included in offerings • Insurers must comply with consumer protections
Public Awarenessof Low Performing Systems and Hospitals • Ratings of hospitals will be readily available on the web • Performance indicators profiled
Moving Forward… • “Growth is the only evidence of life.” • John Henry Newman, Apologia pro vita sua, 1864 • “The wheel of change moves on,and those who were down go upand those who were up go down.” • Jawaharlal Nehru • Get comfortable with change!
ReferencesPricewaterhouseCoopers Health Research Institute HealthCast: The customization of diagnosis, care and cure(March 2010) Between now and 2020, health systems will turn from reactive medicine to proactively understanding and supporting individuals in managing their own health. Many health systems say they deliver patient-centered care, but PwC’s research found only pockets in which this is evidenced. Health organizations remain too focused on their own organizations, not what’s best for the patient. Patient-centered care takes health systems out of their comfort zones, forcing them to integrate people, technologies and organizations that are not part of their current routines. Health Reform: Prospering in a post-reform world(May 2010) While it might be overly dramatic to say that everything has changed with the passage of health reform, it can certainly be said that the health system of tomorrow will not be the same as today. To prosper in the post-reform world, health executives will need to reassess current strategies and find ways to work together. This PwC Health Research Institute report illustrates the mega trends that each health sector will face as a result of health reform, the provisions in the law that are driving them, and recommendations on how organizations can turn these challenges into new opportunities. The New Science of Personalized Medicine(October 2009) This PwC report addresses a key new force the healthcare industry faces - personalized medicine. This force is redefining the health industry and disrupting the business models of healthcare organizations. Every player in the health industry, from pharmaceutical and diagnostics companies to hospitals and primary care providers will have to change the way they relate to consumers if they are to compete in an era of personalized medicine. Retailers, consumer product companies and other players accustomed to marketing directly to consumers may have an advantage in this regard over organizations that traditionally have targeted physicians or businesses. “PricewaterhouseCoopers” and “PwC” refer to PricewaterhouseCoopers LLP, a Delaware limited liability partnership, or, as the context requires, the PricewaterhouseCoopers global network or other member firms of the network, each of which is a separate and independent legal entity.