Download
1 / 1
10 likes | 148 Views
Optimizing Nutrition at Birth in VLBW Infants Robin Bissinger , PhD, NNP-BC; Dave Annibale , MD; Annette Crull , RN; John Cahill, MD; Lauree Pearson MSN, NNP-BC; Sarah Taylor, MD, Carolyn Finch, MS, RD Medical University of South Carolina. BACKGROUND. METHODS.

E N D
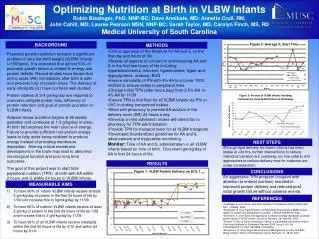
Optimizing Nutrition at Birth in VLBW Infants Robin Bissinger, PhD, NNP-BC; Dave Annibale, MD; Annette Crull, RN; John Cahill, MD; Lauree Pearson MSN, NNP-BC; Sarah Taylor, MD, Carolyn Finch, MS, RD Medical University of South Carolina BACKGROUND METHODS • Critical appraisal of the literature for AA and IL on the first day and hours of life • Review all aspects of concern in administering AA and IL in the first few hours of life including hyperbilirubinemia, infection, hyperkalemia, hyper and hypoglycemia, acidosis, BUN • Ensure osmolality of PN with 4% AA is not over 1000 mOSml to ensure safety in peripheral lines. • Change initial TPN (after hours bag) from 2.5% AA to 4% AA by 11/09 • Ensure TPN is first fluid for all VLBW infants via PIV or UVC including transported babies. • Work with pharmacy to provide AA solution in the delivery room (DR) 24 hours a day • Develop on-line admission orders with direct fax to pharmacy for TPN administration • Provide TPN for transport team for all VLBW transports • Developed Standardized guidelines for AA and IL advancement and triglyceride monitoring. • Monitor: Time of AA and IL administration in all VLBW infants based on time of birth. Document gm/kg/day of AA in first 24 hours of life. Postnatal growth restriction remains a significant problem in very low birth weight (VLBW) infants (<1500gms). It is estimated that almost 50% of postnatal growth failure is related to energy and protein deficits. Recent studies have shown that amino acids (AA) immediately after birth is safe and prevents loss of protein mass. The delivery of early intralipids (IL) have not been well studied. Protein intakes of 3-4 gm/kg/day are required to overcome obligate protein loss, efficiency of protein retention and goal of protein accretion in VLBW infants. Adipose tissue accretion begins at 25 weeks gestation and continues at 1-3 g/kg/day in utero. At birth fat becomes the main source of energy. Failure to provide sufficient non-protein energy leads to fatty acids being oxidized to produce energy instead of providing membrane deposition. Altering critical membrane development in the brain may lead to abnormal neurological function and poor long term outcomes. The goal of this project was to start total parenteral nutrition (TPN) at birth with AA within 2 hours and IL within 24 hours in VLBW infants. NEXT STEPS Although lipid delivery for inborn infants has been stable at <24 hrs, further interventions to reduce individual variation are underway (on line orders) and approaches to reduce delivery time for outborns are under consideration. RESULTS CONCLUSIONS An aggressive TPN program (coupled with attention to enteral nutrition) resulted in improved protein delivery and reduced post-natal growth failure without adverse events. MEASURABLE AIMS To have 90% of inborn VLBW infants receive at least 2 gm/kg/day of protein in the first 24 hours of life by 1/09 and increase this to 3gm/kg/day by 11/09. To have 80% of outborn VLBW infants receive at least 2 gm/kg of protein in the first 24 hours of life by 1/09 and increase this to 3 gm/kg/day by 11/09 To have 90% of all VLBW infants receive intralipids within the first 30 hours of life by 4/10 and within 24 hours by 6/10. REFERENCES • Te Brakke, F. et al. Amino Acid Administration to Premature Infants directly after birth. J Pediatr, 2005. • Poindexter, B. et al. Early Provision of Parenteral Amino Acids in ELBW infants: relation to growth and development outcome. J Pediatr.148:300-5, 2006. • Dinerstein, A. et al. Early and Aggressive nutritional strategy decreases postnatal growth failure in VLBW infants. Journal of Perinatol. 26: 436.442, 2006 • Simmer, K, Rao S. Early introduction of lipids to parenterally-fed preterm infants. Cochrane Database of Systematic Reviews 2005, Issue 2. Art. No. CD005256.DOI:10.1002/14651858. CD005256. • Ehrenkranz, R. Early, Aggressive Nutritional Management for Very Low Birth Weight Infants: What is the Evidence? SeminPerinatol. 31: 48-55, 2007