Download
1 / 1
10 likes | 136 Views
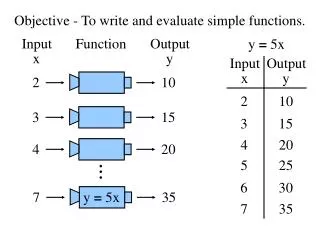
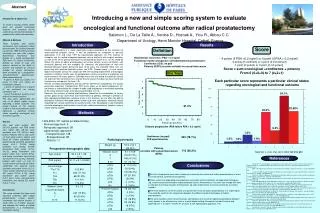
120. 100. 80. 60. 40. 20. 0. 0. 1. 2. 3. 4. 5. 6. 7. Abstract. Score. Definition. Introducing a new and simple scoring system to evaluate oncological and functional outcome after radical prostatectomy

E N D
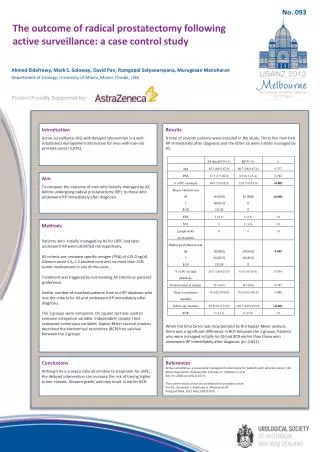
120 100 80 60 40 20 0 0 1 2 3 4 5 6 7 Abstract Score Definition Introducing a new and simple scoring system to evaluate oncological and functional outcome after radical prostatectomy Salomon L., De La Taille A., Vordos D., Hoznek A., Yiou R., Abbou C.C. Department of Urology, Henri Mondor Hospital, Créteil, France Introduction & Objectives To create a scoring system, which takes into account oncological outcome and functional results (continence and erectile function) of patients after radical prostatectomy. Material & Methods Three hundred and eleven consecutive men underwent radical prostatectomy for localized prostate cancer from 1999 to 2004 and were evaluated one year after surgery. Biochemical recurrence was defined as a single postoperative PSA level >0.2 ng/ml. Continence, defined as using no pad, and potency, defined as the ability to achieve and maintain an erection suitable for sexual intercourse, were evaluated by a prospective, self-administered questionnaire. Each patient received - 4 points (if PSA <0.2 ng/ml) or 0 points (if PSA >0.2 ng/ml) for oncological outcome, - 2 points (if continent) or 0 points (if not continent) for urinary continence and - 1 point (if potent) or 0 points (if not potent) for erectile function. The total score represented the sum of all points, higher scores indicating a better outcome. The unique feature of this scoring system is that each particular score represents a particular clinical status regarding oncological and functional outcome. Results One year after surgery, 284 (91.3%) patients had PSA levels <0.2 ng/ml, 243 (78.1%) were continent and 113 (36.3%) were potent. Patients with a total score >4 had good cancer control and could be further subdivided into patients being continent and potent (score 4+2+1, 22.5%), being continent but having erectile dysfunction (ED) (score 4+2+0, 34.1%), being incontinent and potent (score 4+0+1 points 9.3%), and being incontinent and having ED (score 4+0+0, 22.5%). Similarly, patients with score <4 had no cancer control and could be further subdivided into patients being continent and potent (score 0+2+1, 1.9%), being continent but having ED (score 0+2+0 6.1%), being incontinent and potent (score 0+0+1 point, 1.6%), and and being incontinent and having ED (score 0+0+0, 1.2%). Conclusions This score includes the three most important outcomes after radical prostatectomy, cancer control, continence and erectile function. It could allow us to better evaluate and compare the results of radical prostatectomy in a multinational, multicenter setting. pT2 Introduction Results Radical prostatectomy is a major, potentially curative procedure for the treatment of organ-confined prostate cancer. It can be performed by retropubic or perineal approaches (1,2)and since 1997 by laparoscopic approach (3). The majority of urologists use the radical retropubic approach, due to familiarity with surgical anatomy, as well as the nerve sparing technique first described by Walsh et al. (4). As stated by Walsh, the goals of radical prostatectomy are cancer control, urinary continence, and eventually potency with low morbidity (5). However, the presentation of men with localized prostate cancer during the past 10-20 years has changed: More men are presenting with localized prostate cancer, low PSA, Gleason score < 6 and normal digital examination (clinical T1c stage) (6). With the resulting improvement of oncological outcome, functional results such as postoperative urinary continence and potency are major concerns for many patients. Although many men are willing to trade their sexual life and even their continence for a chance to cure cancer, this does not mean that these functions are unimportant for them (7,8). Results of radical prostatectomy (cancer control, continence and potency) are usually presented separately. Postoperative PSA levels allow us to detect progression (9), continence is evaluated by the number of pads used and potency is evaluated according to the status of preservation of neurovascular bundles (10-12). However, the success of radical prostatectomy should be the combination of cancer control, good urinary continence and maintenance of potency. Although a plethora of data regarding postoperative outcome exists in the literature, we are often not able to distinguish if patients with good cancer control also have satisfactory functional results regarding their urinary continence or erectile function (13). We propose a new method to evaluate oncological and functional results after radical prostatectomy together, using a simple scoring system. Biochemical recurrence: PSA > 0.2 ng/ml • 4 points (if PSA <0.2 ng/ml) or 0 point (if PSA > 0.2 ng/ml) • 2 points (if continent) or 0 point (if incontinent) • 1 point (if potent) or 0 point (if not potent) Functional results: prospective self-administered questionnaire: - Continence (ICS): no pad - Potency (IEFF5) erection suitable for sexual intercourse Score = sum oncological +continence + potency From 0 (0+0+0) to 7 (4+2+1) Each particular score represents a particular clinical status regarding oncological and functional outcome One Year 34.1% 91.3% 22.55% 22.5% Methods • 1999-2004: 311 radical prostatectomies • Perineal approach: 9 • Retropubic approach: 58 • Laparoscopic approach: • Transperitoneal: 148 • Extraperitoneal: 85 • Robotic: 11 Disease progression (PSA failure PSA > 0.2 ng/ml) 9.3% 1.2% Continence (no pad) (ICS questionnaire) 243 (78.1%) 1.2% 1.9% 1.6% Pathological results Potency (erection with sexual intercourse) (IIEF5) Preoperative demographic data 113 (36.3%) Salomon L. et al. Eur. Urol. 2003; 44: 656-660 References Conclusions • 1. Young HH. The early diagnosis and radical cure of carcinoma of the prostate: being a study of 40 cases and presentation of a radical operation which was carried out in four cases. Bull Johns Hopkins University 1905;16:315-321. • 2. Millin T. Retropubic prostatectomy: a new extravesical technique. Report on 20 cases. Lancet 1945;2:693-696. • 3. Schuessler WW, Shulam PG, Clayman RV, Kavoussi LR. Laparoscopic radical prostatectomy: initial short term experience. Urology 1997;50:854-857. • 4. Walsh PC, Lepor H, Eggleston JD. Radical prostatectomy with preservation of sexual function: anatomical and pathological considerations. Prostate 1983;4:473-485. • 5. Walsh PC. The status of radical prostatectomy in the United States in 1993. Where do we go from here ? J Urol 1994;152:1816. • 6. Partin AW, Mangold LA, Lamm DM, Walsh PC, Epstein JI, Pearson JD. Contemporary update of prostate cancer staging nomograms (Partin Tables) for the new millenium. Urology 2001;58:843-848. • 7. Fowler FJ, Barry MJ, Lu-Yao G, Wasson J, Roman A, Wennberg J. Effect of radical prostatectomy for prostate cancer on patient quality of life: results from a medicare survey. Urology 1995;45: 1007-1013. • 8. Talcott JA, Rieker P, Propert KJ, Clark JA, Wishnow KI, Loughlin KR, et al. Patient-reported impotence and incontinence after nerve-sparing radical prostatectomy. J Natl Cancer Inst 1997;89:1117-1123. • 9. Pound CR, Partin AW, Epstein JI, Walsh PC. Prostate-Specific Antigen after anatomic radical retropubic prostatectomy. Urol Clin North Am 1997;24:395-406. • 10. Catalona WJ, Carvalhal GF, Mager DE, Smith DS. Potency, continence and complications rates in 1870 consecutive radical retropubic prostatectomies. J Urol 1999;159:433-438. • 11. Quinlan DM, Epstein JI, Carter BS, Walsh PC. Sexual function following radical prostatectomy: influence of preservation of neurovascular bundles. J Urol 1991;145: 998-1002. • 12. Walsh PC, Marschke P, Ricker D, Burnett AL. Patient-reported urinary continence and sexual function after anatomic radical prostatectomy. Urology 2000;55:58-61. • 13. Bianco FJ, Scardino PT, Eastham JA. Radicalprostectomy : long-term cancer control and recovery of sexual and urniray function (« Trifecta ») Urology 2005;66:83-94. • 14. Rassweiler J, Hruza M, Teber D, Li-Ming S. Laparoscopic and Robotic assited radical prostatectomy : Analysis of the results Eur Urol 2006;49:612-624. • We have introduced a score which allows us to evaluate the outcome of radical prostatectomy in terms of cancer control, continence and potency • These results are depending on preoperative evaluation, patient selection, intraoperative techniques (eg. neurovascular preservation) and pathological results. Nevertheless, this score can change with time, as changes the clinical situation of the patient, eg. after improvement of urinary continence or erectile function. • The most important use of this score is to present all results of radical prostatectomy in a single figure, This could be useful for the comparison between the different surgical techniques of radical prostatectomy. • The score could be useful to communicate and compare the results of radical prostatectomy between many centers in an efficient way, even in a multinational setting. Rassweiler tested this score and obtained 22.1% of score 7 and 47.9% of score 6 with laparoscopic approach (14)