Download
1 / 36
360 likes | 376 Views
Learn about the assessment and management of gastro-intestinal symptoms such as constipation, nausea, and vomiting in palliative care patients. Explore pharmacological interventions and other treatment options.

E N D
Managing Gastro-intestinal symptoms Dr Hattie Roebuck, Consultant in Palliative Medicine E mail: harriet.roebuck@colchesterhospital.nhs.uk Dec 2016
Laxatives, PR intervention (BNF classification) Stimulant Softener Na docusate at dose 200mg tds or less Laxido/ movicol Lactulose Mg salts Arachis oil enema Phosphate enemas • Senna • Picosulphate • Bisaccodyl • Glycerine supps
Other options: Relistor • Indications: opioid induced constipation in terminally ill patients who have failed to respond to other laxatives • Methylnaltrexone -dose dependent on weight • Most pts 8 or 12mg s/c 2 doses 24hrs apart • Does not cross Blood brain barrier so analgesic effect of opioids unaffected • Cautions: faecal impaction, diverticular dx, colostomy, peritoneal catheter, liver or renal impairment • C/I: bowel obstruction, perforation • £21 per vial
Nausea vs Vomiting Vomiting post chemo is much better controlled than nausea Molassiotis A et al, Support Care Cancer 2008; 16: 201-8 The evidence for use of anti-emetics is poor ‘A systematic review of the treatment of nausea and/ or vomiting in cancer unrelated to chemotherapy or radiation’ M Davis. JPSM April 2010, Vol 39, no 4, p756
Common causes of N&V in advanced cancer Drugs Gastric stasis Biochemical Intestinal obstruction Other ICP Lichter, 1993
Intractable nausea and vomiting Definition: “Nausea and vomiting that is not adequately controlled after multiple anti-emetics are used in series and/or in combination” Those with the most difficult N&V to manage tend to be those with altered anatomy • eg due to malignant bowel obstruction (dysfunction) or stents/surgical interventions
A general approach - 1 Principles: • 1) Initially - identify and treat reversible causes • This may not be appropriate if someone is imminently dying • 2) Assess severity – does the patient need rehydration • 3) Start anti-emetic treatment • Prescribe regularly • Review control every 24-48 hours • A second line anti-emetic is required in 1/3 of patients 8
A general approach - 2 4) Consider route of administration Oral route maybe ineffective as frequent vomiting = poor absorption Usually -> Syringe driver Community options: • Rectal route: domperidone supps (true/false?) • Buccal prochlorperazine • Hysoscine patch • (granisetron patch) • Olanzapine orodispersible melt = 5mg strength 9
A general approach - 3 • Remember N&V is often multi-factorial • Aim for acceptable control < 3 days • Consider whether dietary/ other factors may help. • Avoiding triggers • Parenteral fluids • Limiting oral intake, protein meals, low fat diet • Relaxation techniques • Acupuncture point P6 • Ginger • Surgery (stents, venting g-tubes), 10
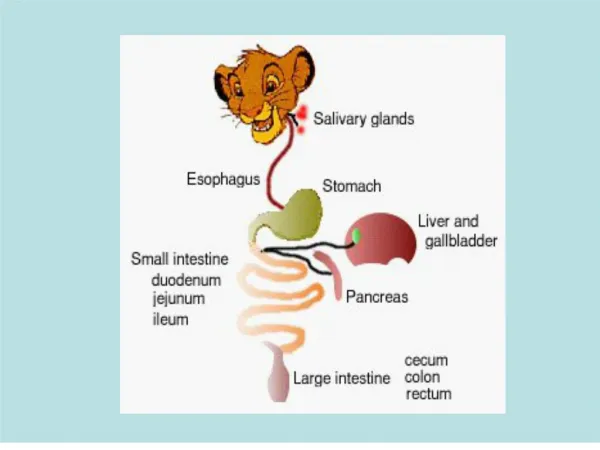
Stomach – usually has slow wave contractions (3/min) • Rate increases with ‘circular vection’ • Vasopressin release • Nausea perception related to vasopressin release • Primates – VP antagonists stop motion sickness • Humans – ginger reduces nausea, vp rise, reduced tachygastria in motion sickness trials
Dietary management • Protein meal – regulates gastrin release, which reduces gastric dysrhythmia & nausea Gastroparesis diet: • Low fat – fat activates stretch receptors in stomach • Fluids • Maintains nutrition & hydration
Fear/Anxiety/ Memory; Meningeal irritation; Raised ICP Drugs; Metabolic products; Bacterial toxins CSF / blood Area Postrema Base 4th ventricle CTZ Cerebral cortex Nucleus Tractus Solitarius Brainstem Vomiting Centre VIII nucleus Peripheral pathways (outside of the CNS) Motion; Labyrinth disorders Autonomic afferents Emesis Mechanical stretch (bowel obstruction or stasis); GI mucosal injury eg RT, chemo; local toxins; drugs
Metoclopramide • Prokinetic • Dopamine 2 antagonist, 5HT4 agonist, 5HT3 antagonist • Central (CTZ) and peripheral action (gut mucosa) • Prokinetic effect antagonised by anticholinergic drugs Side effects Extrapyramidal symptoms Drowsiness, restlessness, depression, diarrhoea • (Max 30mg in 24 hours for up to 5 days – EU review 2013)
Domperidone • Prokinetic • Dopamine 2 antagonist • Acts peripherally and at the CTZ • Does not readily cross the blood brain barrier • Oral only • Side effects • Rarely extrapyramidal • Hyperprolactinaemia • Cardiac arrhythmias • Max dose 10mg TDS (for up to 7 days)
Haloperidol • Dopamine 2 antagonist, 5HT2a and α1antagonist • Acts predominantly at the CTZ but also peripherally (gut mucosa) • First line for biochemical induced N&V • T½ 13 – 35 hours Side effects Extrapyramidal, hyperprolactinaemia Minimal sedation and hypotension NB - Prolongation of QT interval
Cyclizine • H1 antagonist and cholinergic muscarinic antagonist • Acts at the vestibular apparatus (& vomiting centre) • Plasma T½ 13 hours Side effects Drowsiness, urinary retention, dry mouth, blurred vision, constipation, headache, psychomotor impairment • Caution in severe liver disease, severe heart failure, renal failure, glaucoma
Cyclizine • Not advocated for use in heart failure • Increases systemic & pulmonary arterial pressures • Increases right & left ventricular filling pressures • Counteract beneficial haemodynamic effects of opioids in heart failure • ‘Detrimental haemodynamic effects of cyclizine in heart failure’ LB Tan • The Lancet March 1988
Hyoscine Hydrobromide / Butylbromide Hyoscine hydrobromide Hyoscine butylbromide Quaternary ammonium deriv Peripheral AChm antagonist anti-secretory (d of a < 2 hrs) anti-spasmodic Side effects Dry mouth, blurred vision, constipation, urinary retention • Tertiary amine • Central AChm antagonist • anti-emetic • anti-secretory (d of a 1–9 hrs) • anti-spasmodic • Side effects Drowsiness, agitation, delirium, bradycardia
Ondansetron • 5HT3 antagonist • Acts at CTZ and gut mucosa Blocks amplifying effect of excess 5HT on vagus Bowel wall enterochromaffin cells release 5HT by various stimuli. >Sensitises the vagal afferent nerves to emetogenic substances via 5HT3 receptors • Early N&V post chemo: First 24hrs after chemo only • Useful where excessive 5HT released eg chemotherapy or radiotherapy induced damage of gut mucosa, bowel distension, renal failure Side effects Headache, flushing, constipation
Aprepitant • Neurokinin-1 receptor antagonist (NK1) • Substance P found widely in the CNS, including CTZ, VC and GI tract • Chemotherapy increases substance P levels as well as serotonin release • Antiemetic effects of NK1 antagonism is a central effect • Effective for delayed Chemo Induced N&V (>24hrs) • Given alongside 5HT3 antagonist and Dexamethasone • No evidence that it has much role in Palliative Care
Levomepromazine • Dopamine 2 antagonist, Muscarinic cholinergic antagonist, Histamine 1 antagonist, 5HT2A antagonist, alpha-adrenergic antagonist • Acts at vomiting centre • Plasma T½ 15 – 30 hours Side effects Sedation, weakness Dry mouth, hypotension, extrapyramidal symptoms
Olanzapine • Atypical antipsychotic • Dopamine 1, 2, 3 and 4 antagonist 5HT2A, 5HT2C, 5HT3 and 5HT6 antagonist, Alpha-adrenergic antagonist, Histamine-1 antagonist, Muscarinic cholinergic antagonist • Acts at the Vomiting Centre • T½ 34 hours (↑ 52 hours in the elderly) • Side effects Drowsiness, weight gain Dry mouth, constipation, hypotension, peripheral oedema Less movement disorders than with Haloperidol
5HT3 NK1 CSF CTZ D2 Cerebral cortex H1 H1 Vomiting Centre VIII nucleus 5HT2 AChm AChm Autonomic afferents Emesis
Increases ACh production 5HT4 Gastrointestinal Tract D2 5HT3
Dexamethasone • Glucocorticoid • Reduces permeability of the CTZ and the blood brain barrier to emetogenic substances • Reduces neuronal content of GABA in the brain stem • Suggested that antagonism of PGs, release of endorphins and depletion of tryptophan may play a role • ? central or peripheral effect
Summary • Vomiting is unpleasant and debilitating • There are multiple causes • General measures and drug interventions are usually successful • It is helpful to understand the receptor basis of rational prescribing • But we cannot always control all associated symptoms
Medical management of bowel obstruction • Features of bowel obstruction: • Causes of bowel obstruction: • Intraluminal • Extraluminal • Motility disorders (tumour infiltration, neuropathic damage to GIT, drugs such as opioids, anticholinergics etc) • Constipation/ faecal impaction
Systematic review of surgery for malignant bowel obstruction (D. Feuer et al, Gynaecological Oncology 1999) • Control of symptoms 42-80% • Re-obstruction rates 10-50% (most studies did not describe time scales) • Wide range of post op morbidity & mortality Gynaecological Oncology 2003Pothuri et al:palliative bowel obstruction in ovarian ca • Major surgical mobidity 22% - fistula/ abscess/ PE/ peritonitis/ sepsis • Perioperative mortality 6% • But survival mean 12months if palliation successful cf 3 months no surgery
How best to manage? • 1.Surgical opinion & document time for audit • Non surgical: colic/ high risk perforation or no colic • 2. Antiemetic: Stimulant antiemetic/ Non stimulant • 3. Laxative (non stimulant) • 4. Steroid s/c or IV (NNT 6) • 5. NG/ antisecretory • 6. Fluids?
Prognosticating hard Outcomes: • Subacute bowel obstruction can resolve • Most pts will have a recurrence unless have treatment options such as chemotherapy still available to them • Pts can live with subacute bowel obstruction for some months, equates to gut failure • Psycho-social impact can be profound; inability to eat • US – use of parenteral nutrition>UK • Risk of death, sudden deterioration if perforate • Sudden increased pain
Summary • Effect on GIT helpful in determining which laxatives and anti-emetics to use • Adherence to laxative regime can be challenging • Nausea & Vomiting evidence base is poor • Rational prescribing makes sense • Bowel obstruction has significant complications, including death or for chronic subacute bowel obstruction, psycho-social. Equates to gut failure.
Further reading ‘Treating nausea & vomiting in palliative care: a review’ P Glare. Clinical Interventions in Aging 2011; 6 p243 Wood G et al. Management of Intractable Nausea and Vomiting in Patients at the End of Life: “I Was Feeling Nauseous All of the Time…Nothing Was Working” in McPhee S et al (eds) Care at the Close of Life: Evidence and Experience, 2010 www.palliativedrugs.com