Download
1 / 24
260 likes | 427 Views
A Case Study of a Patient with Severe Head Injury. Prepared by: Lady Diana T. Ortega LTIM Department . I. Demographic Data. Name: Patient X Age: 19 years old Sex: Male Nationality: Saudi Marital Status: Single Date of Admission: December 04, 2009.

E N D
A Case Study of a Patient with Severe Head Injury Prepared by: Lady Diana T. Ortega LTIM Department
I. Demographic Data Name: Patient X Age: 19 years old Sex: Male Nationality: Saudi Marital Status: Single Date of Admission: December 04, 2009
II. Physical Assessment Skin warm, slightly moist, smooth, hair evenly distributed Headskull slightly asymmetric, no flaking of scalp, no lesions, no tenderness, scar noted in the craniotomy site, left tempoparietal area Eyes no redness, no discharges, sclera white and clear, pupils reactive to light and accommodation, unable to focus
Nose and Sinuses not perforated, no discharge, NGT is present Mouth no gum bleeding, tongue and uvula in midline position, oral cavity is pinkish in color, buccal mucosa smooth and moist, no ulcers, no swelling, no palpable masses Neck no palpable lymph nodes, trachea on midline position tracheostomy tube is present
Breasts nipples at the same level and protrude slightly, no palpable masses, no nipple discharge Thorax & Lungs thorax is symmetric, no retraction of the Intercostal spaces, no tenderness, back area slightly reddened Upper Extremitiesdecorticate position, arms are unable to extend, abduct and adduct
Nails convex curvature, smooth texture, good capillary refill Abdomen slight abdominal distention, positive bowel sound Lower Extremitiesmalpositioned tibia and fibula, unable to flex, abduct and adduct Genitalia skin of the glans penis is smooth, no ulceration, urethral meatus located ventrally on the end of the penis, no discharge, no palpable masses
IV. Topic Presentation “Head Injury”
Head Injury VI. Etiology Acquired Traumatic Anoxic Hypoxic Closed Open Diffuse Axonal Concussion Contusion Coup Counter coup Penetrating Cerebral edema Confusion,coma, seizure,loss of cognitive & sensory function Increased ICP Decreased cerebral bloodflow Cerebral Ischemia
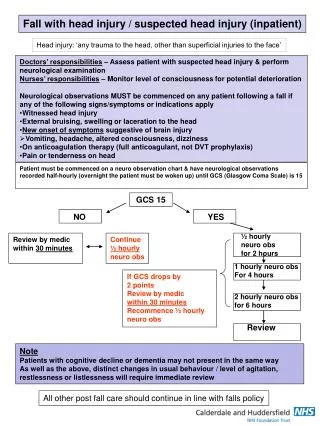
VII. Signs and Symptoms • Prolonged confusion, seizures, and multiple episodes of vomiting • Inability to awaken • dilation of one or both pupils, slurred speech, aphasia, dysarthria, weakness or numbness in the limbs, loss of coordination, confusion, restlessness, or agitation. • do not respond with any body movement to pain, • do not have any speech, and • do not open their eyes.
VIII. Intervention Maintain adequate cerebral blood flow, control increasing ICP by: • Proper Positioning • Hyperventilation • Hypertonic saline • Diuretics • Sedatives, analgesics & paralytics
X. Complications • Brain injury can cause prolonged or permanent effects on consciousness (coma, brain death, vegetative state) • Lying still for long periods may cause many complications • Skull fractures & penetrating injuries may lead to meningitis & abscesses • Complications involving the blood vessels: vasospasm, aneurysms and stroke
XI. Prioritization of nursing problems • Altered cerebral tissue perfusion related to decreased cerebral blood flow secondary to head injury • Ineffective airway clearance related to accumulation of secretions and decreased LOC • Ineffective breathing pattern related to neurological dysfunction • Risk for injury related to disorientation & restlessness • Risk for impaired skin integrity related to immobility
XIII. Nursing Health Teaching Health teaching primarily focused on educating the watcher of care and management: • Review the signs of increased ICP or episodes of seizure with the watcher. • Teach the watcher with the proper techniques: therapeutic use of touch, massage and music • Eliminations of distractions (television, radio, crowds) • Provide one on one communication with the pt. • Provide the necessary education to watcher including proper positioning, ROM exercises and so forth.
XIV. Conclusion Head injury can be mild, moderate or severe. A mild head injury may cause confusion & headache and most people recover from it. A severe head injury may happen if the head is violently shaken without coming in contact with a hard object. When patient recover from moderate to severe head injury they may be left with long term effects such as cognitive disabilities & sensory problems & may lead to long time or maybe permanent bed confinement & sometimes in coma state. In this case, patient needs full time care & management. Comfort should always be consider, support to the back & joints when turning & lifting to prevent strain. Hygiene of the patient, bed & surroundings are also important. A daily bed bath should be given to cleanse, refresh & relax the patient. It also promotes circulation & provides a mild form of exercises. In general, nurses have a big role in assisting these patients in attending their activities of daily living while giving respect to their privacy & dignity.