
Efficacy of Stereotactic Radiosurgery in Treating 1-3 Brain Metastases: A Clinical Study
This study evaluates the effectiveness of stereotactic radiosurgery (SRS) alone for patients with 1-3 newly diagnosed brain metastases, confirmed by MRI. It includes patients with good performance status, excluding those with prior brain radiotherapy or systemic treatment. Treatment was performed using a Linear Accelerator with Dynamic Conformal Arcs, focusing on achieving optimal outcomes in overall survival, local control, and brain disease-free survival (B-DFS). Results indicate that SRS can be a viable option without the need for adjunctive whole-brain radiotherapy in selected cases.

Efficacy of Stereotactic Radiosurgery in Treating 1-3 Brain Metastases: A Clinical Study
E N D
Presentation Transcript
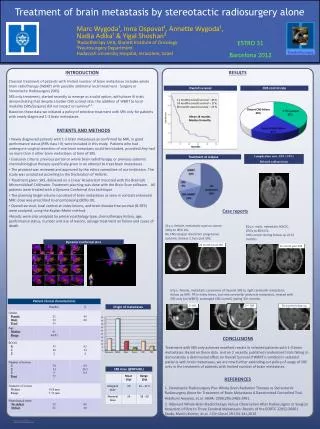
ESTRO 31 Barcelona 2012 Treatment of brain metastasis by stereotactic radiosurgery alone Marc Wygoda¹, Inna Ospovat¹, Annette Wygoda¹, Nadia Adika¹ & Yigal Shoshan² ¹Radiotherapy Unit, Sharett Institute of Oncology ²Neurosurgery Department Hadassah University Hospital, Jerusalem, Israel Newly diagnosed patients with 1-3 brain metastases as confirmed by MRI, in good performance status (RPA class I-II) were included in this study. Patients who had undergone surgical resection of one brain metastasis could be included, provided they had no more than 3 other brain metastases at time of SRS. Exclusion criteria: previous partial or whole brain radiotherapy, or previous systemic chemo/biological therapy specifically given in an attempt to treat brain metastases . The protocol was reviewed and approved by the ethics committee of our institution. The study was conducted according to the Declaration of Helsinki. Treatment given: SRS, delivered on a Linear Accelerator mounted with the BrainLab Micromultileaf Collimator. Treatment planning was done with the Brain Scan software. All patients were treated with a Dynamic Conformal Arcs technique The planning target volume consisted of brain metastases as seen in contrast enhanced MRI: dose was prescribed to encompassing (80%) IDL. Overall survival, local control at index lesions, and brain disease free survival (B-DFS) were analyzed, using the Kaplan-Meier method. Results were also analyzed by primary pathology type, chemotherapy history, age, performance status, number and size of lesions, salvage treatment on failure and cause of death. 1. Stereotactic Radiosurgery Plus Whole-Brain Radiation Therapy vs Stereotactic Radiosurgery Alone for Treatment of Brain Metastases A Randomized Controlled Trial. Hidefumi Aoyama, et.al. JAMA. 2006;295:2483-2491. 2. Adjuvant Whole-Brain Radiotherapy Versus Observation After Radiosurgery or Surgical Resection of One to Three Cerebral Metastases: Results of the EORTC 22952-26001 Study. Martin Kocher, et.al. J Clin Oncol 29:134-141,2010 REFERENCES Classical treatment of patients with limited number of brain metastases includes whole brain radiotherapy (WBRT) with possible additional local treatment - Surgery or Stereotactic Radiosurgery (SRS). SRS only treatment, started recently to emerge as a valid option, with phase III trials demonstrating that despite a better CNS control rate, the addition of WBRT to local modality (SRS/Surgery) did not impact on survival¹⁻². Based on these data we initiated a policy of selective treatment with SRS only for patients with newly diagnosed 1-3 brain metastases. CONCLUSIONS RESULTS PATIENTS AND METHODS INTRODUCTION Treatment with SRS only achieves excellent results in selected patients with 1-3 brain metastases. Based on these data and on 2 recently published randomized trials failing to demonstrate a detrimental effect on Overall Survival if WBRT is omitted in selected patients with brain metastases, we are now further extending our policy of usage of SRS only in the treatment of patients with limited number of brain metastases. Overall survival CNS control rate 12 months overall survival – 41% 24 months overall survival – 17% 36 months overall survival – 13 % Distant CNS failure 44% Mean 14 months Median 9 months months Complication rate: 1/53 (1.9%) Delayed radionecrosis Treatment at relapse 51y.o. female, metastatic ovarian cancer. 20Gy to 80% IDL. No CNS relapse: died from progressive systemic disease 2.5yrs post SRS. Case reports 81y.o. male, metastatic NSCLC. 20Gy to 80% IDL. CNS control during follow up of 15 months. Dynamic Conformal Arcs 15 month post SRS 24 months post SRS 67y.o. female, metastatic carcinoma of thyroid. SRS to right cerebellar metastasis; follow up MRI: PR in index lesion, but new cerebellar peduncle metastasis, treated with SRS only (no WBRT): prolonged CNS control, lasting 33+ months. 30 months follow up 1st SRS 2nd SRS Origin of metastases SRS dose (@80%IDL)





