Download

1 / 13
130 likes | 284 Views
Half of Mechanically Ventilated ICU Patients Could be Served by Assistive Communication Tools. Andrea M. Sciulli, BA Amber E. Barnato*, MD, MPH Jennifer B. Seaman, BSN, RN Melissa Saul, MS

E N D
Half of Mechanically Ventilated ICU Patients Could be Served by Assistive Communication Tools Andrea M. Sciulli, BA Amber E. Barnato*, MD, MPH Jennifer B. Seaman, BSN, RN Melissa Saul, MS Judith A. Tate, PhD, RN Mary Beth Happ, PhD, RN, FAAN University of Pittsburgh School of Nursing and *Medicine
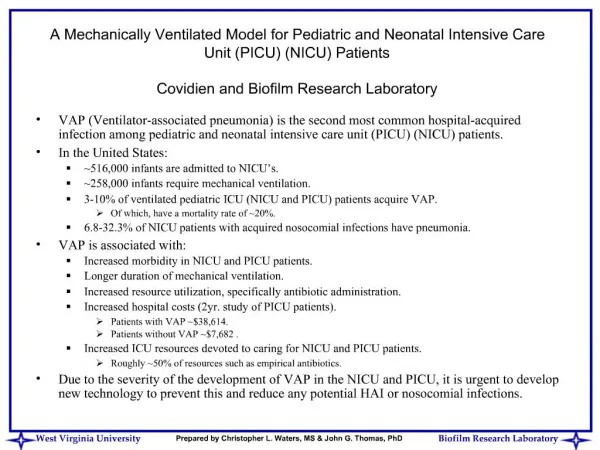
To meet basic communication criteria, ICU patients must be awake, aware, and responsive. • One study of 4 ICUs reported an 18.4% point-prevalence of patients meeting basic communication criteria*. • No studies have documented the proportion of MV patients who are awake, aware, and attempting to communicateusing daily assessments of wakefulness over an entire ICU stay. • BACKGROUND *Thomas LA, Rodriguez CS: Prevalence of sudden speechlessness in critical care units. Clin Nurs Res 2011, 20(4):439-447.
PURPOSE • To determine the longitudinal prevalence of communication ability for at least one 12-hour nursing shift among patients mechanically ventilated for 2 or more days.
SETTING • Stepped wedge crossover cluster randomized trial of nurse training in the use of assistive communication tools. • 6 ICUs in 2 UPMC-affiliated hospitals. • Neurology Neurotrauma • Transplant Trauma • General Medical Cardiovascular • August 1, 2009 – July 31, 2011 [ 24 mos.] • Abstraction occurred across an ICU stay beginning on day 1 and reaching a maximum on day 28. Day 1 was always a MV day.
DATA COLLECTION • Two-stage sampling of medical records and billing data. • Screening for clinical eligibility.
SCREENING/ELIGIBILITY • EMR screening • Medical Archival System billing records • Admissions to a study unit • No prior ICU admission during the current hospitalization • Charge for MV for ≥ 2 days • Random number generator used to number MARS eligibility list • Sequentially screened patients to identify 30 patients/unit/quarter for full EMR abstraction. • Goal of 30 patients/unit/quarter • Goal of 1440 patients upon conclusion of the study (July 2011). • UPMC PowerChart • Nursing note descriptions of alert, arousable, anxious, or awake for ≥ 12-hour period • A score of 6 (Obeys Verbal Commands) for their best motor response on the Glasgow Coma Scale • A score of 1-3 on the Modified Ramsay Scale for sedation • A score of 3-7 on the Riker Sedation-Agitation Scale • MARS eligibility • Clinical eligibility
ENROLLMENT DIAGRAM • *Exclusions: • n = 17 Protected Group • n = 43 Ventilation Location • n = 96 Not 1st ICU Admit • n = 275 Not MV ≥ 2 days, Never vented, On unit < 1 shift
INTERPRETATION • The Neurological ICU had the lowest proportion of MV patients meeting communication criteria 41% • Neuro ICU patients often have insults to the centers of the brain that control communication, comprehension, and/or expression. • Trauma/Cardiovascular ICU’s had the highest proportion 70% • younger patients • shorter periods of MV, post-op ventilations
LIMITATIONS • Sampling from a single region, single academic medical system. • Analysis is limited to MV patients of a 2-day duration, potentially leading to underestimation of longitudinal prevalence of communication ability.
CONCLUSION • Half (53.8%) of MV patients experienced sustained periods of wakefulness during which they were nonvocal, but likely able to communicate in some way.
IMPLICATIONS • A large population of MV patients could be served by assistive communication tools. • Given the large population of MV patients, even small impacts on patient frustration and agitation of assistive communication tools could be clinically significant.