The Hip
The Hip. Joint meeting IBEC & RCSI. Cappagh National Orthopaedic Hospital . Dr. Aamir Shaikh. Clinical Lecturer of Orthopedics RCSI & UCD. 15 th December 2010 . Content:. 1: Anatomy 2: Clinical features. 3: Examination. 4: Pathology. 5: Treatment. Anatomy.

The Hip
E N D
Presentation Transcript
The Hip Joint meeting IBEC & RCSI. Cappagh National Orthopaedic Hospital. Dr. Aamir Shaikh. Clinical Lecturer of Orthopedics RCSI & UCD. 15th December 2010.
Content: • 1: Anatomy • 2: Clinical features. • 3: Examination. • 4: Pathology. • 5: Treatment.
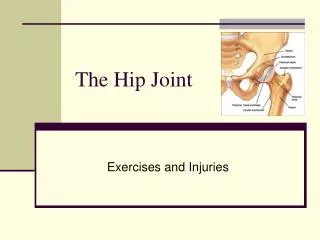
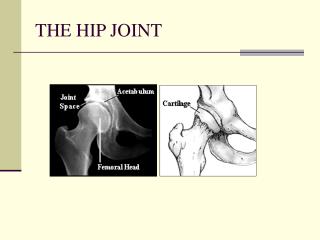
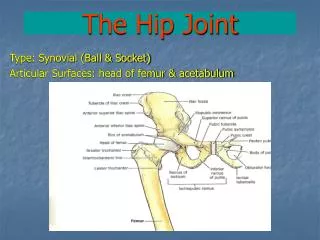
Anatomy. Ball and socket joint of synovial joint. Connects the pelvic girdle to the lower limb Made up of femoral head and acetabulum Designed for stability and wide range of movement Covered with a thin layer of hyaline cartilage
More Anatomy The articular surface of is horse-shoe shaped and is deficient inferiorly- acetabular notch Has a labrum is a circular layer of cartilage which surrounds the outer part of the acetabulum making the socket deeper and so helping provide more stability Acetabular labral tears are a common injury from major or repeated minor trauma
Iliofemoral Ligament This is a strong ligament which connects the pelvis to the femur at the front of the joint It resembles a Y in shape Stabilises the hip by limiting hyperextension
Ligaments. • Pubofemoral ligament • The pubofemoral ligament attaches the part of the pelvis known as the pubis (most forward part, either side of the pubic symphysis) to the femur. • Ischiofemoral ligament: • This is a ligament which reinforces the posterior aspect of the capsule • attaches the ischium to the two trochanters of the femur. • Transverse acetabular Ligament: • Bridges acetabular notch. • Ligament of head of femur: flat and triangular in shape • Lies within joint, ensheathed by synovium
Muscles Gluteals: Gluteus Maximus, Gluteus Minimus and Gluteus Medius Attach to the Ilium and travel laterally to insert into the greater trochanter of the femur Medius and Minimus abduct and medially rotate the hip joint, as well as stabilising the pelvis Gluteus maximus extends and laterally rotates the hip joint
More Muscles Quadriceps The four Quadricep muscles are Vastus lateralis, medialis, intermedius and Rectus femoris All attach inferiorly to the tibial tuberosity Rectus femoris originates at the Anterior Inferior Iliac Spine and acts to flex the hip The 3 other Quad muscles do not cross the hip joint, and attach around the greater trochanter and just below it.
Still More Muscles: Iliopsoas: The is the primary hip flexor muscle which consists of 2 parts Attaches superiorly to the lower part of the spine and the inside of the ilium Cross the hip joint and insert to the lesser trochanter of the femur
Muscles: Hamstrings: The hamstrings are three muscles which form the back of the thigh Attach superiorly to the ischial tuberosity Cause hip extension
Functional Group of Muscles Acting on the Hip Flexors: • Iliopsoas, sartorius, tensor fascia lata, rectus femorus, pectineus, adductor longus, brevis, and magnus, gracilis Extensors: - hamstrings, addcutormagnus, gluteus maximus Adductors: - adductor longus, brevis, and magnus, gracilis, pectineus Abductors: - gluteus medius, minimus, tensor fascia lata External rotators: - obturatorexternus, internus, piriformis, quadratusfemoris, gluteus maximus Internal Rotators: - gluteus medius, minimus, tensor fascia lata.
Nerves Femoral (L2,3,4) Obturator (L2, 3, 4) Sciatic (L4,5, S1, 2,) WHY ARE THESE IMPORTANT??? Referred pain to the knee can hide hip pathology and vis versa
Clinical features of Hip Pathology: • Pain. • Stiffness. • Loss of function. • Crepitations. • Leg length discrepancy.
Pain • Most important reported symptom. • Site: Where? • Anterior hip pain DDx: arthritis, hip flexor strain, iliopsoas bursitis, labral tear • Lateral hip pain DDx: greater trochanteric bursitis, gluteus medius tear, iliotibial band syndrome (athletes), meralgiaparesthetica (an entrapment syndrome of the lateral femoral cutaneous nerve syndrome) • Posterior hip pain DDx: hip extensor and external rotator pathology, degenerative disc disease, spinal stenosis • REFERED PAIN: to knee. hip pathology can be referred to the knee as they share the same nerves!!!! • Just because your patient has hip pain does not mean they have hip pathology....do not forget about referred pain from hernias, aorto-iliac vascular occlusive disease, etc.
The Pain Continues... • Timing: When did it start? • Hours, days, weeks, years • Does it radiate? • Sciatica can run from the hip, down the back of the thigh, into the foot • Radiates to the groin can imply inguinal hernia, groin strain, etc. • What does it feels like? • Sharp: muscle strain/tear, fracture • Dull: OA, RA • Achy: OA, RA, AVN
Pain: • What were they doing when the pain came on? • Did they fall? • fractures, muscle tears, haematomas, etc • Playing sports? • Muscle sprain, labral tear, etc • Prolonged exercise? • OA • Gradual vs sudden? • RA,OA vs. trauma
Pain: • Do they have any aggravating or relieving factors? • OA gets worse as they day goes on and is relieved by rest • Muscle tears/sprains may be exacerbated by certain positions • RA is worse after prolonged periods of rest • If analgesia works, find out what they take and how often!
How does the pain affect their daily life? • How far can they walk? • Difficulty walking up/down stairs? • Are they still able to do their favourite hobbies? • Has their partner noticed their pain limiting them? • Are they taking regular analgesia?
If the pain is manageable this effects your management plan Always opt for conservative measures over surgical ones Use analgesia and physiotherapy/ OT when and where appropriate When necessary offer surgical treatment if appropriate
Inspection Watch the patient walk into the room and sit down - walking aid, limp, uncomfortable gait Inspect hips for scars, swelling, obvious deformity Assess leg length for any true leg length discrepancy (measure from ASIS medial malleolus) and apparent leg length (umbilicus medial malleolus) - a difference in true leg length indicates hip disease on the shorter side - a difference in apparent leg length are due to tilting of the pelvis
Palpate • Mid point of inguinal ligament • hip joint and iliopectinal bursa • Lateral aspect of thigh • trochanteric bursa • Feel for crepitations while hip is moved in I.R / E.R
Movement Test flexion (135 deg): flex knee and move it towards the chest without moving the opposite leg if opposite side moves apply THOMAS TEST (tests for fixed flexion deformity)
More Movement • Rotation (45 deg) -With hip and knee flexed move the foot outward (ext rotation of hip) and inward (int rotation of hip • Abduction (50 deg) Adduction (45 deg): - stand on the same side of the bed as the leg being tested - put your hand over the ASIS of the side not being tested to stabilize the pelvis - with your other hand grasp the heel of the leg being tested and move it outwards as far as possible - then bring the leg across to the opposite side to test adduction • Extension (30 deg): - ask the patient to roll onto their stomach - place one hand over the sacroiliac joint while the other elevate each leg
And the Extra Tests Trendelenburg test: - ask the patient to stand first on one leg then the other - normally the non weight bearing hip rises or stays level - with proximal myopathy or hip joint disease the non weight bearing side sags Neurological exam: -power, tone, sensation Know your nerve supply!!! flexion: L2/3 extension: L5, S½ abduction: L4/5, S1 adduction: L2/3/4
Osteoarthritis Definition: A degenerative joint disease that causes stiffness, pain, and reduction in movement What are the two types? Primary OA: middle aged/ elderly, aetiology unknown Secondary OA: anyone with predisposing factors such as SUFE, CDH, DDH, Perthes, or early onset trauma/ fracture to hip joint etc
OA Pathogenesis Affects weight bearing joint. Prevalence increases with age Disease accelerated by mechanical instability/ stress on jt/increased stress on jt surface initial changes in articular cartilage fibrillation of cartilage vertical clefts exposure of subchondral bone with continuous pressure this leads to sclerosis of subchondral bone (eburnation) bone degeneration under stress creates cysts At joint margins new bone forms resulting in spurs/ osteophytes.
Radiological manifestations: Subchondral Sclerosis.
And this? Spur/ osteophytes.
This one? Sub periosteal Cyst formation. And finally. Bone on bone surface contact.
OA Presentation • Pain: relieved by rest • Stiffness: typically lasting 15-20min then disappears • Joints show reduced movement and is associated with crepitus • Joint swelling/ deformity • Usually affects weight bearing joint • Hip: pain in buttock/upper thigh, limited movement resulting in antalgic gait, hesitant gait to avoid pain • Knee: pain/crepitus at joint surface, deformity results in bow legs/ knock knees • Spine: usually C/L spine, stiffness, radicular pain from compression of spinal nerves • Hands: Heberden’s node, Bouchard’s nodes • Feet: deformity of 1st MT bunion
What to look for on X-rays ? Narrowing of jt space Sclerosis of subcondral bone Cystic bone changes Osteophytes
Treatment: • Conservative • Weight loss • Modify daily activities, walking aids • Physiotherapy • Analgesia: aspirin, paracetamol , NSAIDS + other opioid. • Surgical • Arthroplasty • When patients have severe pain, nocturnal pain, pain at rest, and severely restricted mobility & functional in-capacity. • Arthrodesis • Rarely used in OA, sometimes used in pt too young for hip replacement • Osteotomy • Utilised to realign deformities and spread the transmitted loads more evenly in younger pts
Rheumatoid Arthritis Is a chronic systemic disease of unknown aetiology Characterized by chronic symmetric inflammation of the joints Variable extra articular manifestation F>M 4:1 Genetic prediposition with HLA
RA Pathogenesis • Primarily involve synovial joint • Inflammation synovitis exudation of fluid and inflammatory cells into joint cavity • Inflammation stimulates ingrowth of vessles and proliferation of synovial cells pannus • Pannus secretes lytic enzymes and mediators of inflammation destroys cartilage and erodes underlying bone
RA Presentation • Often insidious but may present with a sudden onset of joint pain, swelling, redness • Early morning stiffness • Symmetrical involvement of small jts • Joint deformity and contracture • Hands: z-deformity, Swan Neck, Boutonnierre, ulnar deviator, subluxation of MC • a/w low grade fever, loss of appetite, malaise, fatigue • Extra articular manifestation: • Lymphadenopathy • Splenomegaly • Subcutaneous nodules • Eyes: scleritis, keratoconjunctivitissicca, Sjogrens syndrome • Lungs: serositis, fibrosis • CVS: pericarditis, pericardial effusion
Investigations • History and Physical Exams • Bloods: FBC (check for anaemia from chronic disease/methotrexate /vit def), ESR, CRP, Rheumatoid Factor • Check uric acid levels to outrule gout • X-rays
What to look for on X-rays Soft tissue swelling Juxta-articular osteopaenia Marginal erosions Joint space narrowing Deformity Hands are often affected earliest
American College of Rheumatology Criteria • morning stiffness • arthritis of 3 or more joint areas • arthritis of hand joints • symmetric arthritis • subcutaneous rheumatoid nodules • serum rheumatoid factor • x-ray finding — periarticular erosions, osteopenia, loss of joint space • A patient has RA if at least 4 criteria are present and the first four for 6 weeks
Treatment • Medical: • NSAIDs • Reduce stiffness and synovitis, improve mobility • do not change outcome • Second Line Tx • Gold salts, penicillamine, immunosuppressants (methotrexate) infliximab (anti tnf-α) • Known as the DMARDs (Disease modifying antirheumatic drugs) • Third Line Tx • Corticosteroids (prednisolone) – lowest dose to control symptoms and minimize side effects • Intra-articular steroids may be utilised in accessible joints
Treatment • Surgical • Early in disease process before significant radiographic changes – synovectomy • Can be performed arthroscopically • Advanced disease • Joint replacement (Arthroplasty) – particularly hip and knee • Restores pain free function • Joint fusion (arthrodesis) – now confined to digital joints, ankle and wrist
Total Hip Replacement: • Prosthetic replacement of arthritic hip joint with metal. • Two components acetabular & Femoral. • Acetabulum shell is either made from poly, X3 or metal with or without option for securing with cancellous screws. • Bearing surface acetabular: UHMW Polyethylene. X3 Poly. With or without 10 deg posterior lip. Ceramic or metal. • Stem use is metal with polish coat or porous coat finish of different offset. • Either cement use on both sides or no cement use sometimes hybrid system is used.
Bone cement : PALACOS-R • Constituents:1: 40.8 gm of powder (polymer) with: Gentamicin 0.5 gm as Gentamicin sulphate. Methyl- methacrylate- methyl acrylate co-polymer Benzoyl peroxide. Zirconium dioxide. Chlorophyll. 2. 18.8 gm of liquid in amber glass ampoule. Methyl methacrylate (stablised with hydroquinone) N-N –dimethyl-p-toluidine Chlorophyll – copper-complex.