Download
1 / 16
180 likes | 339 Views
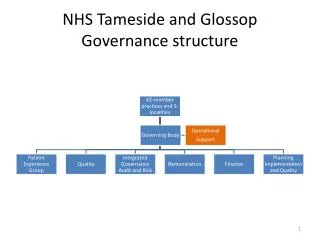
Governance in the NHS. Keith Chantler Associate Medical Director Central Manchester & Manchester Children’s University Hospitals NHS Trust. Aims. What is the NHS trying to achieve? How is this currently being achieved (good & bad points)? What improvements can be made, and by whom?

E N D
Governance in the NHS Keith Chantler Associate Medical Director Central Manchester & Manchester Children’s University Hospitals NHS Trust
Aims • What is the NHS trying to achieve? • How is this currently being achieved (good & bad points)? • What improvements can be made, and by whom? • Not a ‘route map’ - helping industry try to understand what the NHS is trying to achieve
NHS Trusts • All 600 or so Trusts are part of the NHS but the NHS is not a single company • They are required to achieve the same end points:- • Safeguard patients • Minimise risk to organisations (including finances) • How they achieve it is up to each one • They can and will behave differently • For most Trusts, R&D is not a business (but it should be!)
Governance (Broadly the same across the EU) • Patient Safety • Quality • Resources • Defining responsibilities
Why do we need it ? • Science • News headlines against us • Lost public confidence • Participation is optional in a free system (burden) • Costs – direct • UK labour and asset costs are high (for all of us) • Costs – indirect • Govt policy to reduce patient access times – increased R&D may a barrier to clinical tragets/performance • Contractual obligations and liabilities • Litigious society • Slow to change from risk averse – it’s a new world
Governance • Many of the governance arrangements are new to the NHS (risk averse) • Help the R&D managers to understand the risks involved in simple language • Is it a qualitative, non-invasive study? devices
Important Note • NHS governance is also played out in the media, not simply the courts
Patient Safety • Ethics Committees • Locality issues (local knowledge) • Expertise of Principal Investigators (PIs) • Environment • Personal and ‘Team Time’ • Resources • Trust has a Duty of Care to patients - need to know what is proposed to be done by its staff (honorary staff) • R&D Committees • Need to be effective
Joint NHS & University Contracts • Trust and University relationships vary greatly - depends upon the regularity of interaction • Clarify at outset whether they have joint or separate arrangements (improving) • Suggest that a joint approach is used - get one organisation to lead on behalf of both • Trust signs Contract – BUT agreement from both is important (this can vary)
Joint NHS & University Contracts Important points to consider: • Clarify the contract, who with? • Indemnity – who requires what? • Who is leading the costing?
Improving Governance Administration • Don’t ‘contract’ separately with PI from the Trust. • For each study understand who is involved, who makes decisions/signs and time required.
Improving GovernanceR&D Offices • R&D Managers and Staff need more training in legal/contracting, risk management and insurance • Whose responsibility is it to do this? • Individual • Trust – need competent managers • Industry (it’s in your interest?) • What might be Role of NHS R&D Forum • Should provide as service like a Professional Body • Trusts R&D businesses – needs professional managers • R&D Professionals – the ultimate aim
…..continued • Companies are better set up to manage contracts than many Trust R&D offices – you have specialists in:- • Finance • Contracting • Legal • Insurance • Many R&D Offices operate with few staff
Working Together • One contract with Trust or multiple? • Invest the time in order to achieve the best result possible (applies to NHS/Industry) • In general R&D managers have a good working relationship with each other • Use this relationship to reduce set-up administrative burden • All parties should make a concerted effort to use electronic administrative systems
How to improve recruitment? • Feasibility, including local service managers who will know about local circumstances • Note; Employing research staff on income from recruitment is risky and therefore Trusts may have few staff in early stages of contract