Download
1 / 1
10 likes | 57 Views
Non-Hodgkin Lymphoma Showing Abnormalities of c-myc Including Dual Translocations Involving c-myc and Bcl-2: A Clinicopathologic Study. R Jastania, V Kukreti, M AlShraim, D Bailey, B Patterson, M Crump, S Boerner, W Geddie. University of Toronto.

E N D
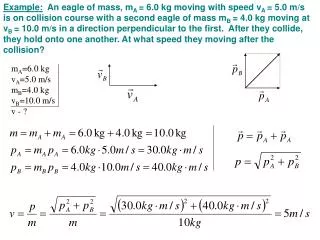
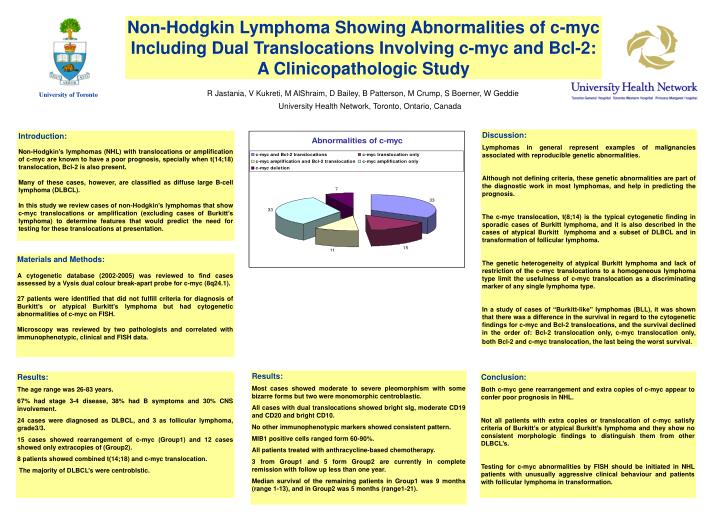
Non-Hodgkin Lymphoma Showing Abnormalities of c-myc Including Dual Translocations Involving c-myc and Bcl-2: A Clinicopathologic Study R Jastania, V Kukreti, M AlShraim, D Bailey, B Patterson, M Crump, S Boerner, W Geddie University of Toronto University Health Network, Toronto, Ontario, Canada Discussion: Lymphomas in general represent examples of malignancies associated with reproducible genetic abnormalities. Although not defining criteria, these genetic abnormalities are part of the diagnostic work in most lymphomas, and help in predicting the prognosis. The c-myc translocation, t(8;14) is the typical cytogenetic finding in sporadic cases of Burkitt lymphoma, and it is also described in the cases of atypical Burkitt lymphoma and a subset of DLBCL and in transformation of follicular lymphoma. The genetic heterogeneity of atypical Burkitt lymphoma and lack of restriction of the c-myc translocations to a homogeneous lymphoma type limit the usefulness of c-myc translocation as a discriminating marker of any single lymphoma type. In a study of cases of “Burkitt-like” lymphomas (BLL), it was shown that there was a difference in the survival in regard to the cytogenetic findings for c-myc and Bcl-2 translocations, and the survival declined in the order of: Bcl-2 translocation only, c-myc translocation only, both Bcl-2 and c-myc translocation, the last being the worst survival. Introduction: Non-Hodgkin’s lymphomas (NHL) with translocations or amplification of c-myc are known to have a poor prognosis, specially when t(14;18) translocation, Bcl-2 is also present. Many of these cases, however, are classified as diffuse large B-cell lymphoma (DLBCL). In this study we review cases of non-Hodgkin’s lymphomas that show c-myc translocations or amplification (excluding cases of Burkitt’s lymphoma) to determine features that would predict the need for testing for these translocations at presentation. Materials and Methods: A cytogenetic database (2002-2005) was reviewed to find cases assessed by a Vysis dual colour break-apart probe for c-myc (8q24.1). 27 patients were identified that did not fulfill criteria for diagnosis of Burkitt’s or atypical Burkitt’s lymphoma but had cytogenetic abnormalities of c-myc on FISH. Microscopy was reviewed by two pathologists and correlated with immunophenotypic, clinical and FISH data. Results: Most cases showed moderate to severe pleomorphism with some bizarre forms but two were monomorphic centroblastic. All cases with dual translocations showed bright sIg, moderate CD19 and CD20 and bright CD10. No other immunophenotypic markers showed consistent pattern. MIB1 positive cells ranged form 60-90%. All patients treated with anthracycline-based chemotherapy. 3 from Group1 and 5 form Group2 are currently in complete remission with follow up less than one year. Median survival of the remaining patients in Group1 was 9 months (range 1-13), and in Group2 was 5 months (range1-21). Results: The age range was 26-83 years. 67% had stage 3-4 disease, 38% had B symptoms and 30% CNS involvement. 24 cases were diagnosed as DLBCL, and 3 as follicular lymphoma, grade3/3. 15 cases showed rearrangement of c-myc (Group1) and 12 cases showed only extracopies of (Group2). 8 patients showed combined t(14;18) and c-myc translocation. The majority of DLBCL’s were centroblstic. Conclusion: Both c-myc gene rearrangement and extra copies of c-myc appear to confer poor prognosis in NHL. Not all patients with extra copies or translocation of c-myc satisfy criteria of Burkitt’s or atypical Burkitt’s lymphoma and they show no consistent morphologic findings to distinguish them from other DLBCL’s. Testing for c-myc abnormalities by FISH should be initiated in NHL patients with unusually aggressive clinical behaviour and patients with follicular lymphoma in transformation.