Download

1 / 12
120 likes | 148 Views
Tubal Ligation (Female Sterilization) Session IIIB Preoperative Client Assessment and Preparation for Minilaparotomy. Objectives. By the end of this session, participants will be able to: State the purpose of preoperative client assessment

E N D
Tubal Ligation (Female Sterilization) Session IIIBPreoperative Client Assessment and Preparation for Minilaparotomy
Objectives By the end of this session, participants will be able to: • State the purpose of preoperative client assessment • List the components of preoperative client assessment • Describe the process of preoperative assessment • List the preoperative instructions given to clients in preparation for minilaparotomy • Demonstrate how to perform client assessment, using tools such as checklists and the MEC • Counsel the client in preparation for surgery • Demonstrate how to prepare the client for minilaparotomy
Why Should We Conduct a Preoperative Assessment? • To determine the client’s physical and emotional fitness for female sterilization by minilaparotomy • To determine whether she has medical conditions that increase risks • To confirm that the client still wishes to receive female sterilization • To prepare the client for surgery under anesthesia
Preoperative Assessment • Who should perform the preoperative assessment? • When should it be performed? • Who is ultimately responsible for making the final client assessment on the day of surgery?
Components of Preoperative Assessment Includes: • Taking a medical history • Performing a physical examination • Carrying out laboratory exams if needed
Taking a Medical History • General information, such as: • Age, occupation, and level of education • Obstetric and gynecologic history: • Number of pregnancies, parity, number of living children, last menstrual period, history of pelvic infection or other sexually transmitted infection, contraceptive use • Medical and surgical history, such as: • Any current medical conditions, respiratory and/or cardiac illness, current medications, allergies, smoking, and alcohol or drug use • Previous surgery (pelvic or abdominal) and previous experience with anesthesia
Performing a Physical Examination • General condition and nutritional status • Weight • Vital signs • Auscultation of the lung and heart • Abdominal examination • Pelvic examination • Other examinations as indicated, including laboratory tests
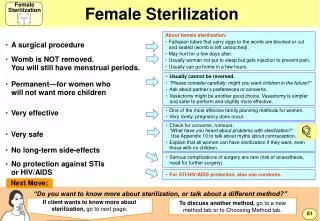
How Can a Provider Be Reasonably Sure that the Client Is Not Pregnant? A provider can be reasonably sure that a woman is not pregnant if she has no symptoms or signs of pregnancy and meets any of the following criteria: • She has not had intercourse since last normal menses. • She has been correctly and consistently using a reliable method of contraception. • She is within the first seven days after normal menses. • She is within four weeks postpartum (for nonlactatingwomen). • She is within the first seven days postabortionor following a miscarriage. • She is fully or nearly fully breastfeeding, amenorrheic, and less than six months postpartum. From: World Health Organization. 2004. Selected Practice Recommendations for Contraceptive Use. Geneva.
Providing Preoperative Instructions to Clients • Preoperative instructions should be given after the assessment. • They should be simple and clear, preferably in a local language. • The provider should ask the client to repeat the instructions. • Additional written (printed) instructions (with illustrations for those who are illiterate) should be provided. • Instructions should include: • What to do a day before surgery • When to come to the clinic • Whether the client needs to be accompanied by a relative to the clinic (to take care of a baby, walk her home, etc.) • What to do after the procedure (wound care, resuming work, sex, etc.) • Warning signs of problems • What to do if she experiences any of the warning signs • A routine return date and where to go for follow-up
Scheduling the Surgery • Clients without any preexisting medical condition that requires special attention can be scheduled at their convenience. • A waiting period of a few days may be beneficial. • In outreach services offering minilaparotomy services, the procedure can be performed on the same day. • Ideally, interval clients should be scheduled during the proliferative phase of the cycle. • Postpartum and postabortion clients should be scheduled within seven daysof their procedure. • After using emergency contraception, a client can be scheduled for surgery within 7 days of next menses.
Verifying Informed Consent • Surgical team must verify that the client has signed the informed consent and understands procedure is permanent and that she can change her mind for LARCs etc. • All to be done before medication with sedatives or other premedication
Supporting the Client Just before the Procedure • Prepare the client emotionally for surgery. • Inform the client: • About the procedure in detail • About the medication she will receive • That she is free to ask questions at any time • If the client seems anxious or nervous, explore her reasons for this. If there are none, reassureher. • Additional supportive activities will be offered by one of the team members.