Download
1 / 122
1.26k likes | 2.48k Views
Therapeutic Hypothermia. Joseph Foley 12-17-2009. Therapeutic Hypothermia. Background. Sudden Cardiac Death Estimated number of out-of-hospital SCD cases is 300,000 per yr in US Incidence anywhere from 35-125/100,000 people with 25% less than 65y/o Cobb JAMA 2002

E N D
TherapeuticHypothermia Joseph Foley 12-17-2009
Therapeutic Hypothermia Background • Sudden Cardiac Death • Estimated number of out-of-hospital SCD cases is 300,000 per yr in US • Incidence anywhere from 35-125/100,000 people with 25% less than 65y/o • Cobb JAMA 2002 • de Vreede-Swagemakers JACC 1997 • If ROSC and admitted, median survival to discharge in US is 7.9% • Lloyd-Jones Circulation 2009 • Favorable outcomes of those admitted to hospital is 11-48% indicating large number of pts who either die or have permanent severe neurological damage • Becker Ann Emer Med 1993 Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Therapeutic Hypothermia Background • Hypothermia • Definition- a condition in which an organism's temperature drops below that required for normal metabolism and body functions. • Subdivided into four different degrees: • Mild (32 - 35ºC or 90 - 95ºF) • Moderate (28 - 32ºC or 82.4 - 90ºF ) • Severe (20 - 28ºC or 68 - 82.4ºF) • Profound ( < 20ºC or < 68ºF) Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Hypothermia in History • History • The Greek physician Hippocrates advocated the packing of wounded soldiers in snow and ice • Hypothermia has played a major role in the success or failure of many military campaigns • Hannibal's loss of nearly half his men in 218 BC while crossing the Alps • Near decimation of Napoleon's armies during Russian Invasion of 1812. • Losses of lives to hypothermia continued in one degree or another through the first and second world wars. • During the second world war Nazi Germany conducted numerous cold experiments on human prisoners. • Civilian examples of deaths caused by hypothermia are found during the sinking RMS Titanic, RMS Lusitania and RMS Empress of Ireland. Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Hypothermia in History Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Hypothermia in Nature Background • Hibernation • A state of inactivity and metabolic depression in animals, characterized by lower body temperature, slower breathing, and lower metabolic rate. • Hibernating animals conserve energy, especially during winter by utilizing body fat as an energy reserves, at a slow metabolic rate and get their energy via gluconeogenesis. • Carey et al. Physiological Reviews 2003. • This slowed metabolic rate is what leads to a reduction in body temperature and not the other way around. • Before entering hibernation most species eat a large amount of food and store energy in fat deposits in order to survive the winter. • Hibernation isn’t continuous and is typically interrupted by sporadic arousals wherein body temperature is restored to normal levels. Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Hypothermia in Nature • Hibernation • Animals that hibernate: • Bats, • Ground squirrels and other rodents, • Mouse lemurs, • The West European Hedgehog, • Monotremes (Echnidas & Platypus) • Marsupials (pygmy-possum). Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Hypothermia in Nature Background • Hibernation • Hibernating ground squirrels may have abdominal temperatures as low as −2.9 °C (27 °F) for more than three weeks at a time, although the temperatures at the head and neck remain at 0 °C or above. • One animal that some famously consider a hibernator is the bear, which actually goes through "denning“ rather than "true hibernation". • During a bear's winter sleep state, the degree of metabolic depression is much less than that observed in smaller mammals and it can be easily aroused. • Body temperature remains relatively stable (depressed from 37 °C (99 °F) to ~ 31 °C (88 °F)) Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Hypothermia in Pop Culture Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Hypothermia in Medicine Background • Cryotherapy • Cryonics • Low-temperature preservation of humans and animals that can no longer be sustained by contemporary medicine until resuscitation may be possible in the future. • Currently, human cryopreservation is not reversible. • The most famous known cryopreserved patient is baseball player Ted Williams • There is a popular urban legend that Walt Disney was cryopreserved but is false because he was actually cremated. 1 on 1 anytime Shaq…bring it! Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Hypothermia in Medicine • Spinal Cord Injuries Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Hypothermia in Medicine • Hypothermia is protective when it is induced before or during an anoxic result • Young RSK, Neurologic outcome in cold water drowning. JAMA 1980. • Hypothermia may act as an anticonvulsant. • Orlowski JP, Hypothermia and barbiturate coma for refractory status epilepticus. Crit Care Med 1984. • Hypothermia decreases cerebral edema after traumatic brain injury • Shiozaki TS, Effect of mild hypothermia on uncontrollable intracranial hypertension after severe head injury. J Neurosurg 1993. • Jagid J, Head cooling decreases brain temperature after traumatic brain injury, Departments of Neurosurgery and Pediatrics*, Miller School of Medicine, University of Miami, 2004. Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Hypothermia in Medicine • Hypothermia is used for cerebral protection during operations involving cardiopulmonary bypass. • Swain JA, Cardiac surgery and the brain. N Engl J Med 1993. • Cardiac Transplantation • Normally a donor's heart is injected with KCl prior to being removed from the donor's body and packed in ice in order to preserve it. • The ice can usually keep the heart fresh for a maximum of 4-6 hours with proper preservation • Cooling an organ from 37 º C to approximately 0 º C slows metabolism by a factor of 12-13 Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Summary • Hypothermia has been used for centuries to treat wounds & preserve organs in a variety of different settings. Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Physiologic Effects of Hypothermia Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Physiologic Effects of Hypothermia • Decreased oxygenation • Shifts oxyhemoglobin-dissociationcurve to left • Vasoconstriction • VQ mismatch • Increased blood viscosity • Metabolicacidosis • Lactate generation due to shiveringand decreased tissue perfusion • Impaired hepaticmetabolism and impaired acid excretion. • Danzl, Accidental hypothermia, N Engl J Med 1994. Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Physiologic Effects of Hypothermia • Dehydration, ileusand fluid shifts with body temperatures below 32 º C. • Electrolyte imbalances. • Hypothermia masks potassium-induced changes in the electrocardiogram. • Cold-induced renalglycosuria • Hematocritincreases 2% per 1 degree º C decline intemperature. • Danzl, Accidental hypothermia, N Engl J Med 1994. Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Physiologic Effects of Hypothermia • Coagulopathies despitenormal clotting factor levels because cold directly inhibits the enzymatic reactions of the coagulationcascade. • Not reflected normal PT or PTT, sincethese tests are routinely performed only at 37 °C. • Platelet activity declines because thromboxaneB2production is temperature-dependent. • Cold-inducedthrombocytopenia from direct BM suppression and hepatosplenic sequestration. • Hypercoagulabilityoccurs with possible thromboembolism. • Danzl, Accidental hypothermia, N Engl J Med 1994. Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Physiologic Effects of Hypothermia • Metabolism is reduced by 5% to 8% per degree Celsius reduction of core temperature. • Decreased neurologic electrical activity and therefore O2 demand and CO production. • Ca++ buffering capacity of cells fails leading to cell death. • Ca++ sequestration is ATP and/or oxygen dependent • Cellular depolarization causes release of glutamate, which further promotes Ca++ influx. • Above processes attenuated by hypothermia. • Siesjo, Ann NY AcadSci 1989 • Busto, Stroke 1989 • Illievich, AnesthAnalg1994 Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Physiologic Effects of Hypothermia • Reperfusion after cardiac arrest with normothermic, oxygenated blood leads to the formation of reactive oxygen species. • Causes cellular damage by lipid peroxidation, DNA toxicity, and induction of apoptosis. • Several studies have shown that hypothermia attenuates oxidative stress and lipid peroxidation. • Globus MY, J Neurochem 1995 • Horiguchi T, J Neurotrauma 2003 • Lei B, Stroke 1994 Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Physiologic Effects of Hypothermia • Functions as immune modulator by inhibiting neutrophil infiltration and function, reducing lipid peroxidation and leukotriene production. • Wang GJ, Neuroscience 2002 • Akriotis V, J Leukoc 1985 • Dempsey RJ, Neurosurgery 1987 • Activation of microglia, which contributes to neuronal injury by production of NO, TNF-α, and glutamate, is mitigated. • Kumar K, Neuroreport 1997 Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Physiologic Effects of Hypothermia • Hypothermia attenuates cytochrome p450 transit, thus the initiation of apoptosis, and subsequent caspaseactivation. • Xu L, J Cereb Blood Flow Metab 2002 • Zhao H, J Cereb Blood Flow Metab 2005 • Fukuda H, Brain Res 2001 • Hypothermia suppresses apoptosis • Antiapoptoticprotein Bcl-2, a potent cell-death suppressor, is enhanced. • Proapoptoticfactor BAX is suppressed. • EberspacherE, ActaAnaesthesiol Scand 2005 • Zhang Z, Brain Res Mol BrainRes 2001 Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Summary • Metabolism is reduced by 5% to 8% for each 1° C decrease in core temperature. • Hypothermia minimizes reperfusion injuries, functions as an immune modulator and prevents apoptosis on a cellular level Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Board Review Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
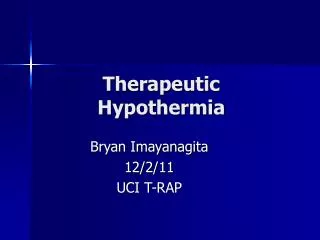
Osborn Waves Background • In 1953, Dr. John Osborn described the J wave as an “injury current” resulting in ventricular fibrillation during experimental hypothermia. • Osborn JJ. Experimental hypothermia: Respiratory and blood pH changes in relation to cardiac function. Am J Physiol 1953. • Hypothermia increases the epicardial to endocardial K+ current during repolarization. • Transmural voltage gradient reflected on ECG as a prominent J, or Osborn, wave. • Differential dx = early Repolarization, Hypercalcemia, and the Brugada syndrome. Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Osborn Waves Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Clinical Data • Williams & Spencer from John Hopkins University • 1958 Annals of Surgery • Case Report • 4 patients, both traumatic and nontraumatic cardiac arrest victims, 2 children, and 2 adults • No-flow times of ~ 5 minutes were resuscitated to favorable neurological outcome with open heart cardiac massage and hypothermia induced with surface cooling after ROSC for 24-72 hours. • The authors stated, • “Patients who show evidence of CNS damage following cardiac resuscitation should be promptly cooled to 32°C to 34°C” Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Clinical Data • Similar case series described again by same group in 1959. • 19 patients with anoxic neurologic injury after in-hospital cardiac arrest and ROSC after open cardiac massage. • 12 patients received hypothermia (30 - 33 ° C) between 1 and 6 hours after cardiac arrest, and 6 survived; • 7 patients did not undergo hypothermia, and 1 survived. • Williams GR Jr, Spencer FC: Clinical use of hypothermia following cardiac arrest. Ann Surg 1959. Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Clinical Data • Peter Safar championed hypothermia for years but it generally laid dormant (or hibernated) until the 1990s. • ClinAnesth 1965 – Management of comatose patient • Crit Care Med 1978 - Resuscitation after global brain ischemia-anoxia • IntAnesthesiolClin 1979 - Pathophysiology and resuscitation after global brain ischemia • Ann Emer Med 1985 - Resuscitation of dogs from cold-water submersion using cardiopulmonary bypass Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Clinical Data • In 1991, dog model of cardiac arrest • 10 minutes of VF followed by 5 minutes of CPR before defibrillation and ROSC • Significant benefit at 72 hours when mild hypothermia was induced within 15 minutes of ROSC and maintained for 60 minutes. • Stertz F, P Safar, et al. Crit Care Med 1991. Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Clinical Data • In a study by Kuboyama, using a dog model, the benefit of hypothermia diminished if induction was delayed by 15 minutes after ROSC. • Histology showed decrease in the neurologic injury despite this delay. • Kuboyama, P Safar, et al.Crit Care Med 1993 Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Clinical Data • Benefits limited with moderate hypothermia <30°C owing to arrhythmias, infections, and coagulation problems. • Danzl, Accidental hypothermia, N Engl J Med 1994. • Animal experiments demonstrated that mild hypothermia (32°C-34°C), was safer than moderate hypothermia and had protective and resuscitative effects on the brain after cardiac arrest. • Sertz, Safar, et al. J Cereb Blood Flow Metab 1990 Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Therapeutic Hypothermia Pilot Study • “Clinical Trial of Induced Hypothermia in Comatose Survivors of Out-of-Hospital Cardia Arrest” • Bernard Ann Emer Med 1997 • Australia, single center Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Bernard Ann Emer Med 1997 Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Bernard Ann Emer Med 1997 Background • Methods • Ice packs used to decrease tympanic temperature to 33 °C. • Intubated, sedated, paralyzed. • Maintained at 33 °C for 12 hours and then rewarmed over 6 hours to 36 °C with heated oxygen and surface heating. • GCS score used to determine neurologic outcomes, no formal neuropsych eval. Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Bernard Ann Emer Med 1997 Background • Results • ROSC in Hypothermia 23.1min vs. Normothermia 25.2min • A core temperature < 34 °C reached at mean of 74 minutes after ROSC. • No significant complications from hypothermia. • Sepsis, coagulopathy, neutropenia, thrombocytopenia • At 72hrs, if fully conscious were transferred to the CCU unless still intubated or critically ill. • Pts hemodynamically stable but still comatose at 72hrs underwent trach/PEG. • Pts deeply comatose, with unreactive pupils and multisystem organ dysfunction, were considered to have a hopeless prognosis, and active therapy was withdrawn. Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Bernard Ann Emer Med 1997 Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Randomized Clinical Trials Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
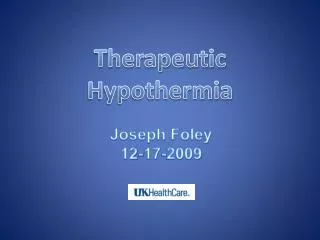
Bernard NEJM 2002 • Australian, multicenter • Randomized on odd and even days & not blinded*** Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Bernard NEJM 2002 Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Bernard NEJM 2002 • Methods • Cooling began pre-hospital with ice packs. • Maintained at 33 °C for 12 hours and then rewarmed over 6 hours to 36 °C. • ASA for all, Heparin/Thrombolytics & if angioplasty indicated • All received Lidocainegtt x 24hrs • Pts formally assessed by rehab Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Bernard NEJM 2002 Background Home Physiology Rehab Clinical Data Long-Term Facility PublishedReviews Long-Term Facility UK Protocol Conclusions
Bernard NEJM 2002 Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Bernard NEJM 2002 Background Physiology Clinical Data 49% 26% p=0.046 ARR = 23% NNT = 4.3 PublishedReviews UK Protocol Conclusions
Bernard NEJM 2002 • Results • ROSC • Hypothermia 26.5min vs. Normothermia 25.0min • Core temperature reached goal at 120min • Nonsignificant mortality rates • Hypothermia group 22/43 (51 %) vs. normothermiagroup 23/34 (68 %) (P=0.145) • The primary cause of death was cardiac • 5/22 in hypothermia group • 4/23 in normothermiagroup • Remaining deaths in both groups primarily from severe neurologic injury and withdrawal of care. Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
Randomized Clinical Trials Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
HACA NEJM 2002 • Austria, Randomized • Physicians responsible for assessing neurologic outcome within the first six months after the arrest were unaware of the treatment assignments. Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
HACA NEJM 2002 Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
HACA NEJM 2002 Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions
HACA NEJM 2002 • Methods • Hypothermia group cooled to target temp 32 - 34°C within 4 hrs of ROSC using an external cooling mattress, ice packs if unsuccessful. • Temperature maintained at 32 - 34°C for 24 hours, followed by passive rewarming over 8 hrs. • Tympanic then bladder temperature Background Physiology Clinical Data PublishedReviews UK Protocol Conclusions