Download
1 / 35
350 likes | 491 Views
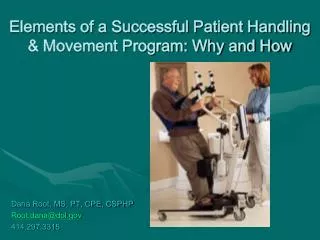
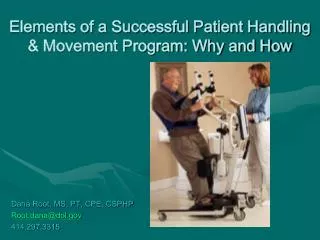
Patient Handling and Movement Programs (PHAMP): Building the Business Case. Arizona Society for Healthcare Risk Management. Merl Miller, CIE; Certified Industrial Ergonomist Ashton Tiffany, LLC. Prepared by :. Healthcare Has Changed…. But… Not Enough. Prepared by :.

E N D
Patient Handling and Movement Programs (PHAMP): Building the Business Case Arizona Society for Healthcare Risk Management Merl Miller, CIE; Certified Industrial Ergonomist Ashton Tiffany, LLC Prepared by :
Healthcare Has Changed… But… Not Enough Prepared by :
Why Do We Need a Business Case? • Dissatisfaction with current state • Shared recognition of the need for, and logic of, SPHM • Need for SPHM as a combination of threats and opportunities ‘Urgency’ to build momentum for acceptance of SPHM Prepared by :
Categories of Value Prepared by :
QualityCare Patient Satisfaction Staff Satisfaction
Reduce Exposure to Hazards Injury rates Injury frequency Lost workdays Restricted workdays Direct cost of injuries Indirect cost Total cost Prepared by :
Personal Protective Equipment Yet, we routinely accept exposureto musculoskeletal hazards. Prepared by :
Incident Cost Iceberg • INJURY & ILLNESS • DIRECT COSTS • Medical • Compensation costs • INDIRECT COSTS • Overtime • Quality • Patient injury • Hiring/Retraining • Short-term disability • Productivity/Efficiency • Underreporting Prepared by :
Closer View of WRMSDs REACTIVE APPROACH Lagging Indicators CRITICAL (Disability) SEVERE (Surgery) SERIOUS (Incident) MAJOR (Pain) MINOR (Discomfort) UNRECOGNIZED (Tasks) PROACTIVE APPROACH Leading Indicators Ergonomic Risk Factors Prepared by :
Replacement Staff vs. Core Staff • What do we know about core staff? • Who is providing bedside care? • How does it impact quality? • Is this effective or efficient? Prepared by :
Magnet® Recognition Program Culture of Safety: EP30. Describe and demonstrate “The structure(s) and process(es) used by the organization to improve workplace safety for nurses based on standards such as the ANA’s Safe Patient Handling and Movement” Ref: ANCC (2008) The Magnet Model Components and Sources of Evidence. ANCC, Silver Spring, MD, p.19. Prepared by :
Improve Patient Quality Patient experience Length of stay Never events Negative patient outcome: falls, skin and respiratory health Prepared by :
Staffing Prepared by :
Patient Outcome Patient Experience Prepared by :
Immobility • Functional decline • Reasons for patient immobility • Consequences of patient immobility • respiratory (pneumonia) • CV (DVT, hypotension) • GI (constipation) • musculoskeletal • skin (pressure ulcers) • psychosocial Prepared by :
Understanding the Value • Reduced patient falls and associated costs • Reduced patient ulcers and treatment costs • Increased patient satisfaction • Reduced costs from WC and lost/ restricted workdays • Improved worker satisfaction • Improved worker retention and reduced turnover Prepared by :
Systems and Processes • Efficiency • number of staff to do task? • time spent waiting for assistance? • Non–value added tasks • Wasted motion and physical effort • Barriers to efficiency Prepared by :
What is Necessary for Change to Occur? Model to follow—implementation process: • outlines the organizational strategy • provides an understandable approach • organizes tools and resources Focus on process! Prepared by :
Barriers to Efficiency Equipment access: Location Distance Compliance Inventory and par levels: Insufficient resources Budget Accountability Logistics and cleaning: Shrinkage Schedule Turnaround time Prepared by :
What are the Program Elements? • Leadership commitment • Employee involvement and participation • Program management and coordination • Worksite analysis • Risk identification, analysis, and control • Education and training • Medical management • Continuous monitoring and improvement Prepared by :
Employee Engagement Develop a facility SPHM team • facility process leader(s) • administrative sponsor • SPHM specialist or coordinator • SPHM team members • SPHM coaches • ergonomics and injury prevention specialist Prepared by :
Why Do You Need a SPHM Specialist? • Strong and committed leadership • Visible, active, and public commitment/ support • Willingness to take initiative and challenge the status quo • High level of attention to/focus on SPHM • Change leadership as full-time activity Prepared by :
Financial Performance Net operating margin Retention Labor costs (float, pool, and travelers) Workers’ compensation premiums: based on frequency and severity Prepared by :
Loss Data Used to Build a Shared Need • Forces any resistance or apathy to be addressed head-on • Indicates why SPHM is critical • Builds momentum to get SPHM program communicated and launched Prepared by :
Gaining Commitment • Identify direct and indirect cost of WRMSDs • Calculate overtime, premium labor and agency staff • Relate to operations and profit margin • Link with patient safety and satisfaction • Consider the dollars of reimbursement needed to offset workers’ compensation claims? Prepared by :
Return on Investment • Productivity • Efficiency • Performance • Injury risk • Probability of injury • Injury consequence Prepared by :
Operating Margin Impact Prepared by :
Indirect Costs 3–10 X Direct Costs
Operating Margin Impact Prepared by :
Operating Margin Impact How many additional surgical cases must be performed to cover these dollars? Prepared by :
Which Option Makes Sense? Prepared by :
External Organizations with Recognition • The Joint Commission Accreditation • ANCC Magnet Recognition Program® • American Nurses Association • American Industrial Hygiene Association • Association of periOperative Registered Nurses • National Association of Orthopaedic Nurses • American Association for Safe Patient Handling and Movement Prepared by :
Regulations • Safe patient handling—federal bill introduced • States with legislation passed or introduced • TX, IL, MN, MD, NJ, RI, WA, NY, HI, MA, MI, MO, VT • Federal OSHA—general duty clause: “every employer must provide a safe working environment for their employees” Prepared by :
If you have questions or would like a copy of this presentation, please contact:Merl Miller, CIE Ashton Tiffany, LLC 333 E. Osborn Road, Suite 300 Phoenix, Arizona 85012602.222.3840merl.miller@ashtontiffany.comhttp://www.ashtontiffany.com Prepared by :