Taking the gastro- intestinal history
440 likes | 685 Views
Taking the gastro- intestinal history. Dr. J.A. Coetser Department of Internal Medicine CoetserJA@ufs.ac.za. SOCRATES. Site Onset Character Radiation Alleviating factors Timing Exacerbating factors Severity. Presenting symptoms: Abdominal pain. Site

Taking the gastro- intestinal history
E N D
Presentation Transcript
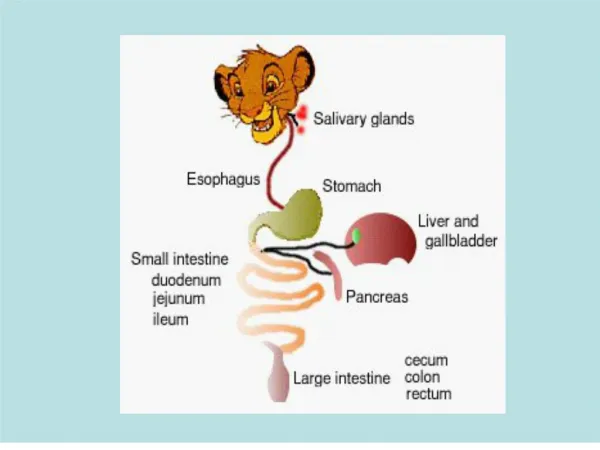
Taking the gastro-intestinal history Dr. J.A. Coetser Department of Internal Medicine CoetserJA@ufs.ac.za
SOCRATES • Site • Onset • Character • Radiation • Alleviating factors • Timing • Exacerbating factors • Severity
Presenting symptoms:Abdominal pain • Site • Where is the maximum intensity of the pain? • Parietal peritoneum involvement gives very localized pain • E.g. appendicitis
Presenting symptoms:Abdominal pain • Onset • Is pain acute or chronic? • When did it begin? • How often does it occur?
Presenting symptoms:Abdominal pain • Character and pattern • Colicky or steady? • Colicky pain due to peristaltic movements • Bowel obstruction • Urethers
Presenting symptoms:Abdominal pain • Radiation • To the back = pancreatic disease / peptic ulcer • To the shoulder = diaphragmatic • To the neck = oesophageal reflux
Presenting symptoms:Abdominal pain • Alleviating factors • Antacids may relieve peptic ulcer or reflux pain • Defaecation or passing of flatus may relieve pain from colon disease • Rolling around may relieve colicky pain • Lying very still may relieve pain from peritonitis
Presenting symptoms:Abdominal pain • Timing • Pain from peptic ulceration may be related to meals • Ask about the daily pattern of pain
Presenting symptoms:Abdominal pain • Exacerbating factors • Eating may precipitate ischaemic pain or pancreatic pain • Coffee, alcohol, spicy food may exacerbate reflux
Presenting symptoms:Abdominal pain • Dull or burning epigastric • pain • Episodic • May occur at night, may • wake patient • Pain often unrelated to • meals • Pattern of peptic ulcer disease pain
Presenting symptoms:Abdominal pain • Pattern of pancreatic pain • Epigastric pain • Relieved by sitting up and leaning forward • Pain often radiates to back • Vomiting often associated
Presenting symptoms:Abdominal pain • Pattern of biliary pain • Rarely colicky • Epigastric pain with cystic duct obstruction • Usually severe, constant for hours • History of similar episodes in past • If cholecystitis develops, pain can shift to right hypochondrium
Presenting symptoms:Abdominal pain • Pattern of renal colic pain • Colicky pain superimposed on background of constant pain in renal angle • Often radiates to groin
Presenting symptoms:Abdominal pain • Pattern of bowel obstruction pain • Colicky pain • If obstruction is in small bowel, pain often periumbilical • Colonic pain can occur anywhere • Small bowel obstruction colic cycles every 2-3 minutes • Large bowel obstruction colic cycles every 10-15 minutes • Obstruction often associated with vomiting, constipation, and abdominal distension
Presenting symptoms:Appetite and weight change • Anorexia + weight loss • Consider malignancy • Depression could also be a cause • Increased appetite + weight loss • Malabsorption of nutrients • Thyrotoxicosis • Liver disease may cause disturbance of taste
Presenting symptoms:Early satiation and postprandial fullness • Early satiation can be due to gastric diseases • Gastric cancer • Peptic ulcer
Presenting symptoms:Nausea and vomiting • Causes • GIT infections, e.g. S.aureus • Small bowel obstruction • Pregnancy • Drugs (digoxin, opiates, dopamine agonists, chemotherapy) • Peptic ulcer disease with gastric outlet obstruction • Gastroparesis from e.g. diabetes mellitus • Acute hepatobiliary disease • Alcoholism • Psychogenic vomiting • Eating disorders e.g. bulimia • Raised intracranial pressure
Presenting symptoms:Nausea and vomiting • Timing of vomiting • Delayed >1h after meal = gastric outlet obstruction • Early morning vomiting = pregnancy, raised intracranial pressure, alcoholism • Contents of vomitus • Bile = connection between stomach and duodenum • Old food = gastric outlet obstruction • Blood = ulceration
Presenting symptoms:Heartburn and acid regurgitation • Heartburn • Retrosternal burning pain or discomfort, due to inappropriate relaxation of lower oesophageal sphincter • Aggravated by bending or lying down • Relieved by antacids • Acid regurgitation • Sour or bitter tasting fluid coming up into mouth • Waterbrash • Excessive secretion of saliva into mouth, associated with peptic ulcer disease or oesophagitis
Presenting symptoms:Dysphagia • Dysphagia = difficulty in swallowing • Can occur with solids or liquids • Odynophagia = painful swallowing • Causes • Infectious oesophagitis • Peptic ulceration • Caustic damage to oesophagus • Ask patient to point to site where food gets stuck
Presenting symptoms:Dysphagia • Dysphagia + heartburn = possible stricture formation • Dysphagia only with 1st few swallows = lower oesophageal ring / oesophageal spasm • Progressive dysphagia for solids = stricture / carcinoma / achalasia • Dysphagia for both solids and liquids = motor disorders, e.g. achalasia
Presenting symptoms:Diarrhoea • Increased frequency of stools (>3 per day) • Change in consistency, loose and watery • Distinguish between acute and chronic diarrhoea
Presenting symptoms:Diarrhoea Secretory Osmotic Abnormal intestinal motility Exudative Malabsorption
Presenting symptoms:Diarrhoea • Secretory diarrhoea • High volume • Persists when patient fasts • Occurs when secretion in GIT exceeds absorption, e.g. cholera • Osmotic diarrhoea • Large volume stools • Disappears with fasting • Occurs due to excessive solute drag, e.g. lactose intolerance • Abnormal intestinal motility • E.g. thyrotoxicosis, irritable bowel syndrome
Presenting symptoms:Diarrhoea • Exudative diarrhoea • Small volume stools, but frequent • Associated blood or mucus • E.g. inflammatory bowel disease • Malabsorption • Can result in steatorrhoea = fatty, pale colored, extremely smelly, floating, difficult to flush away • >7g fat in 24h stool
Presenting symptoms:Constipation • May refer to: • Frequency <3/week • Hard consistency • Straining to evacuate stools • Causes: • Drugs • Metabolic • Endocrine • Neurological • Malignancy • Pregnancy • Perineal problems
Presenting symptoms:Constipation • Irritable bowel syndrome • Can present with alternating constipation and diarrhoea • No structural or biochemical abnormality • Abdominal pain plus 2 or more: • Pain relieved by defecation • Looser or more frequent stools with onset of abdominal pain • Mucus per rectum • Feeling of incomplete emptying of rectum • Visible abdominal distension
Presenting symptoms:Mucus Solitary rectal ulcer Fistula Villous adenoma Irritable bowel syndrome
Presenting symptoms:Bleeding • Haematemesis • Vomiting of blood (coffee-ground vomitus) • Ensure this is not from a nose bleed, bleeding tooth socket or coughing up of blood • Usually from source proximal to or at duodenum • E.g. peptic ulcer disease • Mallory-Weiss tear due to repeated vomiting
Presenting symptoms:Bleeding • Haematochezia • Bright red blood per rectum • Blood usually not mixed with stool, found in toilet bowl • E.g. haemorrhoids, local anorectal diseases
Presenting symptoms:Bleeding • Melaena stools • Black, offensive, tarry stools • Bleeding from upper GIT • Massive rectal bleeding • From distal colon or rectum • Angiodysplasia • Diverticular disease
Angiodysplasia • Diverticular disease
Presenting symptoms:Jaundice • Excess bilirubin deposited in skin and sclerae • Ask about colour of urine and stools • If pale stools and dark urine = obstructive or cholestatic jaundice • Stercobilinogen unable to reach intestine • Ask about abdominal pain • Gallstones can cause biliary pain
Presenting symptoms • Pruritis • Itching of skin • Cholestatic liver disease often causes pruritis, worse over limbs • Abdominal bloating and swelling • Bloating due to excess gas or irritable bowel syndrome • Persistent swelling due to ascites • Lethargy • Chronic liver disease • Anaemia
Treatment history • Drugs indicated in GIT disease: • NSAIDs = peptic ulcer disease • Anticholinergic drugs = constipation • Isoniazid = drug hepatitis • Rifampicin = drug cholestasis • Anabolic steroids or contraceptives = cholestasis / peliosishepatis • Paracetamol = liver necrosis
Past history • Surgical procedures can result in jaundice • Anaesthesia e.g. halothane • Hypoxaemia of liver cells causing ischaemic hepatitis • Damage to bile duct during surgery • History of relapsing and remitting epigastric pain, now with acute abdomen = perforated peptic ulcer • Past history of inflammatory bowel disease
Social history Occupation, e.g. exposure to hepatitis Toxin exposure, e.g. vinyl chloride Travel history Alcohol history Contact with someone who had jaundice Sexual history Injections, e.g. intravenous drugs, transfusions, dental treatment, tattooing
Family history Colon cancer and familial polyps Inflammatory bowel disease Coeliac disease