Download
1 / 30
300 likes | 367 Views
Learn the prevalence, risk factors, types, detection methods, treatment options, and prognosis of breast cancer, a common malignancy in women. Discover how early detection and individualized therapy are crucial for improved survival rates.

E N D
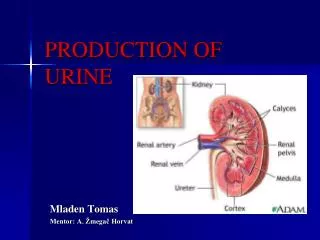
Presented by: Katarina Bojanić Mentor: A. Žmegač Horvat
FACTS & EPIDEMIOLOGY • Most common malignancy in women (25-30%) • 2nd leading cause of cancer deaths(after lung c.) • > 570,000 newcases worldwide eachyear • 2,300 new cases >800 deaths in Croatia (2005)
Oneout ofeight womenwill be diagnosed • Strikes a small percentage of men • ≈1,500 new cases expected to be diagnosed in men next year
Every three minutes a woman in the US is diagnosed with BC • Every 12 minutes a woman dies from BC • All women are at risk (rare in women <40; 10% of palpable masses malignant)
Female Breast Anatomy • Each breast = 15 to20 sections (lobes) arranged like petals of daisy • Inside lobe = smaller structures (lobules) • End of each lobule = tiny sacs (bulbs), produce milk
Lobes, lobules, bulbs- linked by network of thin tubes (ducts) • Carry milk: bulbs → dark area of skin (areola) Duct Areola
Gender Age, Race Family/Personalhistory of BC Genetic factors Menstrual history Certain types of breast disease Radiation Weight (obesity) Exercise Alcohol Reproductive history Hormone replacement therapy Oral contraceptive use Breastfeeding Risk Factors Nonmodifiable risks Modifiable risks
Genetic risk factors →10% of BC familial (hereditary) • BRCA 1&BRCA 2→ tumorsuppressor genes (breast cancer gene) →role in cellular DNA repair →mutation increasesrisk • P53, RAS, C-MYC, RB gene
Types of Breast Cancer Invasive Cancers Noninvasive Cancers(in situ) spread from ducts or lobes into fatty tissue limited to ducts or lobes & does not spread into fatty tissue
Detection methods • Self breast exam • Clinical examination • Mammography > 35 Ultrasound < 35 • Biopsy if indicated
Mammography • X-ray picture of the breast to detect breast cancer • Detects a breast lump before it can be felt
BIOPSY RESULTS • 80% of all breast biopsies turn out to be benign
Clinical Breast Exam • Performed by doctor • Every 3 y. for women 20 – 39 • Yearly for women > 40 yrs of age
Breast Self-Exam Monthly starting at the age of 20! • Still menstruating • 2-3 days after period ends • No longer menstruating • same day every month
Two parts of BSE 1) Visual 2) Palpatory: • Examine each breast separately • Use pads of middle three fingers;feel the texture • Examine the armpits
Visual: Most common: Lump or thickening in breast. Often painless Discharge or bleeding. Redness or pitting of skin over the breast; like the skin of an orange. Change in size or contours of breast. Change in color or appearance of areola.
Abnormal Breast Changes Lump in the breast Changes in breast size of shape Notify Your Doctor Nipple discharged or tenderness Changes in the skin of the breast
TREATMENT OPTIONS & PROGNOSIS • Depend on • Size of the tumor • Invasive or in situ • Histologic type - ductal (85%) vs. lobular • Estrogen/progesterone receptors (60-70%positive) • Her-2/ neu status (receptor for epidermal growth f.) tm size increases- chance decreases SURVIVAL
Lymph node status • Spread to other parts of the body (bones, liver, lung, brain) • Age (premenopausal = poor prognostic factor)
TREATMENT Goals Cure, Control, Palliation • Surgery • Radiation Therapy (local) • Chemotherapy (systemic) • Hormonal Therapy (systemic) • Immunotherapy Therapy is individualized
SURGERY • Mastectomy (complete/radical) • Breast conservation (partial)
RADIATION THERAPY Local control of disease Indications: • Adjuvant(after partial mastectomy) • Young patients with DCIS • High risk of local recurrence • High energy rays used to kill cancer cells
CHEMOTHERAPY Anticancer drugs = systemic control of disease Indications: • After surgery to reduce risk of recurrence • Large + locally advanced cancer to reduce the size prior to surgery(neoadjuvant) • Metastatic - to reduce cancer that has spread + relieve symptoms & prolong life
HORMONAL THERAPY • Hormones (blood stream) → attach ca.cells, promote their growth • Block the receptor or production of hormones ! • Side effects: hot flashes, depression, ↑risk of uterine cancer, induced manopause, blood clots • Tamoxifen, aromatase inhibitors...
IMMUNOTHERAPY Monoclonal antibodies • Trastuzumab/Herceptin • Patients whose cancer cells over-express Her-2-neu oncogene as measured byIHC or FISH (25 to 30% of patients)
Through early detection and improved treatments more women than ever are surviving breast cancer...
THANK YOU FOR YOUR ATTENTION! Questions ?
References: Kusić Z.Onkologija.Zagreb,2008 Damjanov I, Jukić S, Nola M.Patologija.Medicinska naklada,Zagreb, 2008 Kumar P, Clark M.Clinical Medicine.Saunders Elsevier,London,2007 www.cancer.org www.cancer.gov