Download
1 / 1
10 likes | 133 Views
Topiramate Induced Bilateral Vision Loss William Gartlan OMS IV Rowan University School of Osteopathic Medicine. Chief Complaint – Vision Loss. Intraocular Pressures and Visual Acuity. History of Present Illness

E N D
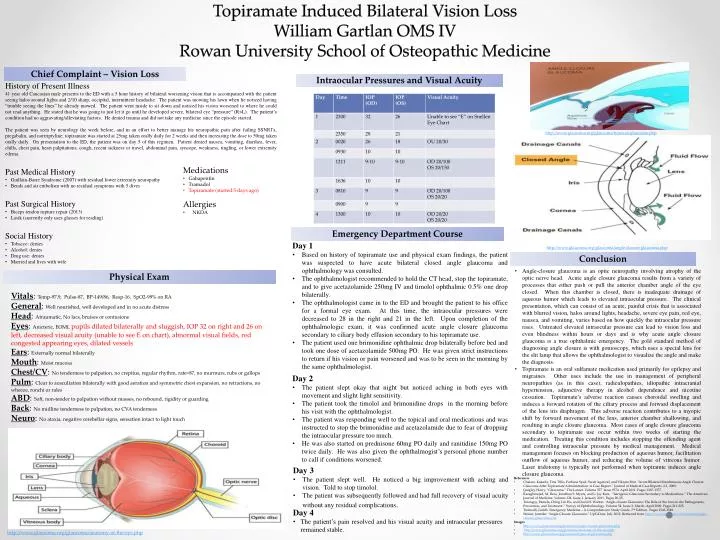
Topiramate Induced Bilateral Vision Loss William Gartlan OMS IV Rowan University School of Osteopathic Medicine Chief Complaint – Vision Loss Intraocular Pressures and Visual Acuity • History of Present Illness • 41 year old Caucasian male presents to the ED with a 5 hour history of bilateral worsening vision that is accompanied with the patient seeing halos around lights and 2/10 sharp, occipital, intermittent headache. The patient was mowing his lawn when he noticed having “trouble seeing the lines” he already mowed. The patient went inside to sit down and noticed his vision worsened to where he could not read anything. He stated that he was going to just let it go until he developed severe, bilateral eye “pressure” (R>L). The patient’s condition had no aggravating/alleviating factors. He denied trauma and did not take any medicine since the episode started. • The patient was seen by neurology the week before, and in an effort to better manage his neuropathic pain after failing SSNRI’s, pregabalin, and nortriptyline; topiramate was started at 25mg taken orally daily for 2 weeks and then increasing the dose to 50mg taken orally daily. On presentation to the ED, the patient was on day 5 of this regimen. Patient denied nausea, vomiting, diarrhea, fever, chills, chest pain, heart palpitations, cough, recent sickness or travel, abdominal pain, syncope, weakness, tingling, or lower extremity edema. • Past Medical History • Guillain-Barre Syndrome (2007) with residual lower extremity neuropathy • Bends and air embolism with no residual symptoms with 5 dives • Past Surgical History • Biceps tendon rupture repair (2013) • Lasik (currently only uses glasses for reading) • Social History • Tobacco: denies • Alcohol: denies • Drug use: denies • Married and lives with wife • http://www.glaucoma.org/glaucoma/types-of-glaucoma.php • Medications • Gabapentin • Tramadol • Topiramate (started 5 days ago) • Allergies • NKDA Emergency Department Course • Day 1 • Based on history of topiramate use and physical exam findings, the patient was suspected to have acute bilateral closed angle glaucoma and ophthalmology was consulted. • The ophthalmologist recommended to hold the CT head, stop the topiramate, and to give acetazolamide 250mg IV and timolol ophthalmic 0.5% one drop bilaterally. • The ophthalmologist came in to the ED and brought the patient to his office for a formal eye exam. At this time, the intraocular pressures were decreased to 28 in the right and 21 in the left. Upon completion of the ophthalmologic exam, it was confirmed acute angle closure glaucoma secondary to ciliary body effusion secondary to his topiramate use. • The patient used one brimonidine ophthalmic drop bilaterally before bed and took one dose of acetazolamide 500mg PO. He was given strict instructions to return if his vision or pain worsened and was to be seen in the morning by the same ophthalmologist. • http://www.glaucoma.org/glaucoma/angle-closure-glaucoma.php Conclusion • Angle-closure glaucoma is an optic neuropathy involving atrophy of the optic nerve head. Acute angle closure glaucoma results from a variety of processes that either push or pull the anterior chamber angle of the eye closed. When this chamber is closed, there is inadequate drainage of aqueous humor which leads to elevated intraocular pressure. The clinical presentation, which can consist of an acute, painful crisis that is associated with blurred vision, halos around lights, headache, severe eye pain, red eye, nausea, and vomiting, varies based on how quickly the intraocular pressure rises. Untreated elevated intraocular pressure can lead to vision loss and even blindness within hours or days and is why acute angle closure glaucoma is a true ophthalmic emergency. The gold standard method of diagnosing angle closure is with gonioscopy, which uses a special lens for the slit lamp that allows the ophthalmologist to visualize the angle and make the diagnosis. • Topiramate is an oral sulfamate medication used primarily for epilepsy and migraines. Other uses include the use in management of peripheral neuropathies (as in this case), radiculopathies, idiopathic intracranial hypertension, adjunctive therapy in alcohol dependence and nicotine cessation. Topiramate’s adverse reaction causes choroidal swelling and induces a forward rotation of the ciliary process and forward displacement of the lens iris diaphragm. This adverse reaction contributes to a myopic shift by forward movement of the lens, anterior chamber shallowing, and resulting in angle closure glaucoma. Most cases of angle closure glaucoma secondary to topiramate use occur within two weeks of starting the medication. Treating this condition includes stopping the offending agent and controlling intraocular pressure by medical management. Medical management focuses on blocking production of aqueous humor, facilitation outflow of aqueous humor, and reducing the volume of vitreous humor. Laser iridotomy is typically not performed when topiramte induces angle closure glaucoma. Physical Exam Vitals: Temp-97.9, Pulse-87, BP-149/86, Resp-16, SpO2-99% on RA General: Well nourished, well developed and in no acute distress Head: Atraumatic, No lacs, bruises or contusions Eyes: Anicteric, EOMI, pupils dilated bilaterally and sluggish, IOP 32 on right and 26 on left, decreased visual acuity (unable to see E on chart), abnormal visual fields, red congested appearing eyes, dilated vessels Ears: Externally normal bilaterally Mouth: Moist mucosa Chest/CV: No tenderness to palpation, no crepitus, regular rhythm, rate=87, no murmurs, rubs or gallops Pulm: Clear to auscultation bilaterally with good aeration and symmetric chest expansion, no retractions, no wheeze, ronchior rales ABD: Soft, non-tender to palpation without masses, no rebound, rigidity or guarding Back: No midline tenderness to palpation, no CVA tenderness Neuro: No ataxia, negative cerebellar signs, sensation intact to light touch • Day 2 • The patient slept okay that night but noticed aching in both eyes with movement and slight light sensitivity. • The patient took the timolol and brimonidine drops in the morning before his visit with the ophthalmologist. • The patient was responding well to the topical and oral medications and was instructed to stop the brimonidine and acetazolamide due to fear of dropping the intraocular pressure too much. • He was also started on prednisone 60mg PO daily and ranitidine 150mg PO twice daily. He was also given the ophthalmogist’s personal phone number to call if conditions worsened. • Day 3 • The patient slept well. He noticed a big improvement with aching and vision. Told to stop timolol. • The patient was subsequently followed and had full recovery of visual acuity without any residual complications. • References • Chalam, Kakarla, Tina Tillis, Farhana Syed, Swati Agarwal, and VikramBrar. “Acute Bilateral Simultaneous Angle Closure Glaucoma After Topiramate Administration: A Case Report.” Journal of Medical Case Reports. 2:1. 2008. • Quigley, Harry. “Glaucoma.” The Lancet. Volume 377. Issue 9774. April 2011. Pages 1367-1377. • Razeghinejad, M. Reza, Jonathan S. Myers, and L. Jay Katz. “Iatrogenic Glaucoma Secondary to Medications.” The American Journal of Medicine. Volume 124. Issue 1. January 2011, Pages 20-25. • Tarongoy, Pamela, Ching Lin Ho, and David S. Walton. “Angle-closure Glaucoma: The Role of the Lens in the Pathogenesis, Prevention, and Treatment.” Survey of Ophthalmology. Volume 54. Issue 2. March–April 2009. Pages 211-225. • Tintinalli, Judith. Emergency Medicine – A Comprehensive Study Guide. 7th Edition. Pages 1543-1549. • Weizer, Jennifer. “Angle-Closure Glaucoma.” UpToDate. July 2012. Retrieved from http://www.uptodate.com/contents/angle-closure-glaucoma.com • Images • http://www.glaucoma.org/glaucoma/angle-closure-glaucoma.php • http://www.glaucoma.org/glaucoma/anatomy-of-the-eye.php • http://www.glaucoma.org/glaucoma/types-of-glaucoma.php • Day 4 • The patient’s pain resolved and his visual acuity and intraocular pressures remained stable. • http://www.glaucoma.org/glaucoma/anatomy-of-the-eye.php