Treatment with hypertonic saline solutions
370 likes | 949 Views
Treatment with hypertonic saline solutions. Øyvind Skraastad Barneanestesiteamet, Rikshospitalet Oslo. 20 years of research and clinical trials. Hypertonic saline,7.5 % NaCl (HS) Hypertonic saline/ 6 % dextrane 70 (HSD) Hypertonic saline/ 6 % HES 200/0.5 (HSS). Hypertonic saline.

Treatment with hypertonic saline solutions
E N D
Presentation Transcript
Treatment with hypertonic saline solutions Øyvind Skraastad Barneanestesiteamet, Rikshospitalet Oslo
20 years of research and clinical trials • Hypertonic saline,7.5 % NaCl (HS) • Hypertonic saline/ 6 % dextrane 70 (HSD) • Hypertonic saline/ 6 % HES 200/0.5 (HSS)
Hypertonic saline • Small volume - 4ml/kg • Infusion in peripheral veins - no phlebitis observed • Colloids added (dextrane,starch) improves volume-expansion - duration • Acute hypovolemia and shock • Mobilisation of extravasal fluid
Hypertonic saline- experimental data and clinical trials • Experimental studies • acute bleeding • sepsis, burns • increased intracranial pressure • Clinical studies • acute traumatology • intraoperative hypovolemia, cardiac surgery
Cardiac output HSD Dextrane HS No volume resuscitation Bleeding Bolusinf. hypotension after infusion baseline minutes Smith -89
To be preferred in volume resucitation • Hypertonic saline solutions should be: • Effective • Increased intravascular volume, increased cardiac output • Duration of effect • Reduced mortality/morbidity • Side effects/adverse effects negliable • Price
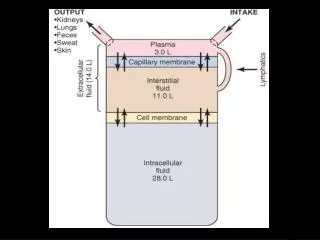
Transcapillary fluid transport Pkap Starling -balance NF = K( Pkap -Pint +int -kap) int Pint P kap = Intravascular hydrostatisk pressure P int = Extravasc hydrostatisk pressure kap = Intravascular colloid osmotisk pressure int = Intravasc. colloid osmotisk pressure kap ions proteins
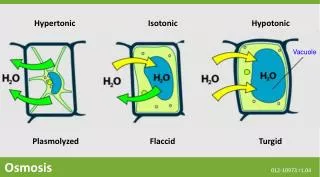
Physiological effects • Transcapillary Osmotic forces Increased plasma volume 1 mOsm excerts osmotisk pressure of 19,3 mmHg Capillary leakage reduce the effect of hypertonic saline, but still Absorbtive force of 50 -200 mmHg (Colloids: 2-4 mmHg)
Osmotic transcapillary fluid transport • Osmotic effects depends on: • permeability for each solute in different capillary beds • number of particles on each side of the membrane • Osmotic effects by: • few, large molecules with low permeability • many, small particles with higher permeability
Effects of hypertonic saline solutions • Intravasation of fluid from extravascular space • Peripheral vasodilatation • Increased cardiac contractility • Increased cardiac index
Other effects • Increased diuresis • Reduced intracranail pressure • Reduced endothelial edema, Reduced precapillary resistance and increased microcirculation • Immunology ? (leucocyte adhesion, mediators of inflammation )
Future of hypertonic saline solutions • Effective fluid resucitation - rapid intravascular rehydration • ”Fluid drug” to reduce extravascular fluid in hypervolemia • After cardiac surgery • Intracranial hypertension
Plasma volum increase ml ekspansion ml infusion Kramer et al. -89 Time
Dilution by 4ml/kg HSDHealthy volunteers Plasmavol 7,6 ml/kg Hb (g/100 ml) Plasmavol 9,7 ml/kg* HSD Time (min) Tølløfsrud et al.-98
Distribution of fluid HSD 4 ml/kg(140ml) minutter Tølløfsrud et al. -00
Distribution of fluid Ringer 25ml/kg (929 ml) Tølløfsrud et al. -00
Relative intravascular volume HSD 4 ml/kg ml expansion ml infusion Ringer 25 ml/kg Infusion Tid (min) Tølløfsrud et al.-00
Relative volume-expansion-effect of HSD/Ringer VEE ratio of HSD/Ringer infusion Time (min) Tølløfsrud et al.-00
Acute traumatology • Effect in patients with multitrauma incl head trauma • Reduced need for infusions • Reduced need for transfusions • No significant hypernatremia, coagulopathy • But hyperchloremia
Cardiac surgery Ex.corp circulation and capillary leakage Ex.vasc.space Cell Ringer Blood Lymph Leakage 11-30 ml/min during ex.corp circulation Koller et al. 1992 Fluid overload at end op.: 5,2 l Tølløfsrud et al 1995
Diuresis and heart surgery ml Inf Tølløfsrud et al. -98
Fluid balance and heart surgery ml Infusion Tølløfsrud et al. -98
Hemodynamic data CI Inf. Tølløfsrud et al. -98
Open heart surgery • Increased CI postoperatively • Reduced SVR • Reduced fluid overload after surgery • But: - increased preload - heart failure • NB !Doses of fluid and rate of infusion
Intracranial hypertension • Continously high sodium values (145-160 mmol/l) may reduce elevated ICP when conventional treatment fails • Reduce transcapillary leak in pathological brain tissue (trauma, tumor, ischemia) ? • Reduce extravascular fluid in areas with normal blood-brain-barrier
Clinical use of hypertonic saline solutions • Optimal dose ? • Optimal rate of infusion ? • Dose bolus 4 ml/kg 5-20 minutes. • NB ! • Volume sensitive patients • vasodilatation • changes in Na- concentration
Conclusion • Safe and effective treatment of hypovolemia • Effective treatment of extravascular fluid overload ? • Beneficial for patients with elevated ICP ?