Download
1 / 40
400 likes | 553 Views
Methodology used for the production of the Canadian. 2007 Canadian Hypertension Education Program. CHEP recommendations are based on critically evaluated clinical trial evidence and highly value improved patient outcomes

E N D
2007 Canadian Hypertension Education Program • CHEP recommendations are based on critically evaluated clinical trial evidence and highly value improved patient outcomes • Use of CHEP recommendations in clinical practice requires an integration of the recommendations with • Individual patient characteristics and preferences • A consideration of the costs of therapy
2007 Canadian Hypertension Education Program Slide kits, clinical practice algorithms and supporting literature for full recommendations can be downloaded from www.hypertension.ca
Canadian Recommendations for the Management of Hypertension • Canada has had annually updated evidence-based recommendations since 1999. • The CHEP process was initiated in 2000 as part of a national strategy to improve blood pressure control in Canada. • The 2000 process was linked to the periodic update of lifestyle and hypertension management recommendations in 1999. • The production of recommendations are linked a separate and specific implementation plan and to an evaluation strategy.
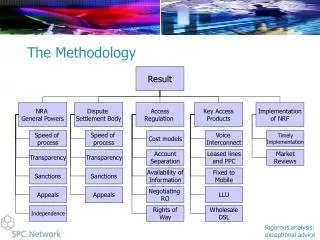
Steering Committee CHEP Organizational Chart Executive Committee Evidence-Based Recommendations Task Force ________________ Central Review Committee Topic subgroups Topic subgroups Topic subgroups Topic subgroups Outcomes Research Task Force Implementation Task Force
Canadian Hypertension Education Program 2007 STEERING COMMITTEE: N Campbell (Chair), M Lebel (CHS), R Petrella (CFPC, BP Canada), S Samis (HSFC), G Taylor (PHAC), S Matheson (CCCN), L Poirier (CPA), D Drouin, J Kaczorowski, J Onysko, S Tobe, R Touyz EXECUTIVE COMMITTEE: N Campbell (Chair), D Drouin, J Kaczorowski, J Onysko, S Tobe, R Touyz (to 2006) R Lewanczuk (from 2006) CENTRAL REVIEW COMMITTEE:B Hemmelgarn (Co-Chair), F McAlister (Co-Chair), N Khan, R Padwal, M Hill, J Mahon
Sponsoring organizations and partners • Sponsoring organizations • Canadian Hypertension Society • Blood Pressure Canada • Public Health Agency of Canada • Heart and Stroke Foundation of Canada • College of Family Physicians of Canada • Canadian Council of Cardiovascular Nurses • Canadian Pharmacy Association • Partner organizations • Canadian Cardiovascular Society • Canadian Society of Nephrology • Canadian Stroke Network • Canadian Society of Internal Medicine • Kidney Foundation of Canada • Volunteers (>90)
Financial Support CHEP is financially supported by the Public Health Agency of Canada and the Canadian Hypertension Society. CHEP receives indirect support from the Heart and Stroke Foundation and Blood Pressure Canada CHEP outcomes studies have been supported by the Public Health Agency of Canada, Canadian Institute for Health Research and the Heart and Stroke Foundation
CHEP - MINIMIZING BIAS CHEP recognizes bias as a serious threat to recommendations processes and takes multiple steps to reduce its impact. Overt steps taken to reduce bias include. • A history of requiring a high level of evidence with patient outcomes for pharmacotherapy recommendations • A centralized systematic literature review • Multiple members in subgroups to represent different views
CHEP- MINIMIZING BIAS • A Central Review Committee (CRC) that is ‘free of COI’ to oversee the evaluation of evidence, development of recommendations and to present the evidence/ recommendations • Overt written disclosure of potential COI at the time of the development of the recommendations • A consensus approach to the drafting of the recommendations chaired by the CRC • Voting on recommendations with the removal of recommendations voted against by 30% of members.
CHEP- MINIMIZING BIAS • Themes, key messages and major implementation tools are developed through a consensus of the full executive. Other internal implementation tools require the consensus of two members of the executive. • External implementation tools must be completely consistent with the content and intent of CHEP recommendations and require a consensus of 3 members of the executive. The CHEP executive prioritized minimizing the potential impact of bias at it’s business planning retreat in May 2006.
METHODOLOGYthe production of recommendations Can J Cardiol 2006;22:559-64
Canadian Hypertension Education Program Recommendations Task Force:S Tobe (Chair), R Lewanczuk (Vice-chair) Accurate Measurement of BP: C Abbott (Chair), K Mann, L Cloutier Adherence Strategies for Patients: R Feldman (Chair), A Milot; J Stone, T Campbell Follow-up of BP: P Bolli (Chair), G Tremblay Risk Assessment: S Grover (Chair), G Tremblay, A Milot Self-measurement of BP: D McKay (Chair), A Chockalingam Ambulatory BP Monitoring: M Myers (Chair), S Rabkin, M Dawes Routine Laboratory Testing: T Wilson (Chair); B Penner, E Burgess Echocardiography: G Honos (Chair) Lifestyle Modification: R Touyz (Chair), N Campbell, N Gledhill,R Petrella, L Trudeau Pharmacotherapy of Hypertension in Patients Without Other Compelling Indications: F McAlister (Chair), G Carruthers, J DeChamplain, G Fodor, P Hamet, R Herman, G Pylypchuk Pharmacotherapy for Hypertension in patients with Cardiovascular Disease: S Rabkin (Chair), M Arnold, G Moe, Jean-Martin Boulanger Diabetes: P Larochelle (Chair), L Leiter, R Ogilvie, C Jones, S Tobe, V Woo, P McFarlane Renal and Renovascular HTN: S Tobe (Chair), B Culleton, K Burns, M Ruzicka Endocrine forms of hypertension: E Schiffrin (Chair) Vascular Protection: R Feldman (Chair), R Hegele, P McFarlane
Evidence Based Recommendations Task Force Subgroups • Office Measurement of BP • Follow-up of BP • Risk Assessment • Self-measurement of BP • Ambulatory BP Monitoring • Routine Laboratory Testing • Echocardiography • Lifestyle Modification • Pharmacotherapy of Hypertension in Patients Without Other Compelling Indications • Pharmacotherapy for Hypertension in patients with Cardiovascular Disease • Diabetes and Hypertension • Renal and Renovascular Hypertension • Endocrine forms of Hypertension • Concordance Strategies for Patients • Vascular Protection
2007 Canadian Hypertension Education Program : The process • Subgroups systematically review the literature using a Cochrane librarian and supplement the search with personal files to Sept 2006 • Application of an evidence-based grading scheme • Use of a Central Review Committee comprised of methodologists to improve consistency of grading • 1 day conference to discuss recommendations and evidence (Sept 2006) • National presentation of draft recommendations (Canadian Cardiovascular Congress Vancouver, Oct 2006) • Voting and ratification of recommendations achieving >70% acceptance
2007 Canadian Hypertension Education Program Detailed methodology of the system to grade evidence can be found in Can J Cardiol 2006;22:559-64
Level of evidence used by the CHEP (2000) Grade Internal validity Precision Applicability Adequate randomized controlled trial (RCT) or subgroup analysis OR systematic review of adequate RCT with similar Rx arms Statistically significant results OR adequate statistical power to exclude clinically important differences Clinically relevant mortality or morbidity outcome measure and representative population A Adequate RCT or subgroup analysis OR systematic review of similar RCT using similar Rx arms Inadequate statistical power to exclude clinically important differences OR systematic review with heterogeneity Validated surrogate outcome measure OR extrapolation of results from another population B Inadequate RCT or subgroup analysis OR cohort/case controlled studies OR systematic review of RCT with Rx arms from different studies Studies in which the 95% confidence intervals do not exclude meaningful contrary conclusions Validated surrogate outcome measure OR extrapolation of results from another population C D None of the above None of the above None of the above
METHODOLOGYthe implementation of recommendations Can J Cardiol 2006;22:595-98
2007 Canadian Hypertension Education Program Implementation Task Force:D Drouin (Chair), J Kaczorowski (Vice-chair) Nurses Sub-group: Jo-Anne Costello, Kori Kingsbury, Sandra Matheson Pharmacists Sub-group: Luc Poirier, Bill Semchuk, Ross Tsuyuki Family Physicians Sub-group: Martin Dawes, John Hickey, Rob Petrella Members at large: Jean-Martin Boulanger, Norm Gledhill, Ross Feldman, Norm Campbell, Sheldon Tobe, Alain Milot, Guy Tremblay, Rhian Touyz, Jay Onysko, Rick Ward
2007 Canadian Hypertension Education Program • An important function of the CHEP executive is the development and updating of key CHEP implementation tools • Implementation of CHEP recommendations is a task for all CHEP members
2007 Canadian Hypertension Education Program • Between 2001 and 2005, The College of Family Physicians of Canada, The Canadian Pharmacy Association and the Canadian Council of Cardiovascular Nurses joined the CHEP steering committee to oversee the integrity and relevance of the process for their disciplines and to aid dissemination • In 2005 specific subgroups of nurses, pharmacists and family doctors were formed to tailor the tools and messages to their discipline and develop dissemination strategies and networks within their discipline.
Some annual dissemination initiatives • Key messages and themes are updated annually • Publications (3-4 summaries plus full scientific documents) with more than 40 publications by or on CHEP in 2006 • CHEP pocket cards (140000) and booklets (10-20000) • Dissemination through the websites • Wall posters • CHEP's "Train the Trainer" Sessions
Some annual dissemination initiatives • Management algorithms • Power point slide sets • Palm application • Endorsement or co-development of education programs with RxD companies • Media releases with HSF • Development of HCP networks (family doctors, nurses and pharmacists)
2007 Canadian Hypertension Education Program A slide kit and other educational resources can be downloaded from http://www.hypertension.ca
Explanation, Statement, or List Important comment, Warning Recommendation Do not Do not 2007 Canadian Hypertension Education Program In the slide kit, special color codes have been associated with specific types of information. Here are some examples: Reminder A red flag is been posted where recommendations were updated for 2007.
Multidisciplinary Executive Summaries Canadian Hypertension Recommendations. “What’ new and what’s old but still important”. One page - clinical 4 page - clinical 6 page - scientific
METHODOLOGYthe evaluation of recommendations Can J Cardiol 2006;22:556-558
Outcomes Research Task Force • An Outcomes Research Task Force was developed to assess the impact of CHEP on hypertension management • Details of the Task force can be found in Can J Cardiol 2006;22:556-558
2007 Canadian Hypertension Education Program Outcomes Research Task Force:N Campbell (Chair), J Onysko (Vice-chair)
Outcomes Research Task Force ORTF Collaborative effort with PHAC, Statistics Canada, provinces and organizations to develop a national surveillance system for hypertension • Physical Measures Surveys • IMS Health Compuscript data • Provincial Administrative Databases • National Questionnaire Surveys (CCHS, NPHS) • National Hospitalization and Mortality Data
Physical Measures Surveys • Ontario HSF will have results of an Ontario physical measures survey assessing hypertension prevalence, awareness, treatment and control in 2007 • Statistics Canada will have results of a national physical measures survey assessing hypertension prevalence, awareness, treatment and control in 2009
Changes in antihypertensive prescriptions in Ontario using IMS Compuscript data Hypertension 2006; 47:22-28
Changes in initiation of antihypertensive prescriptions in elderly Ontarians using provincial administrative data Hypertension 2006; 47:22-28
National Questionnaire Surveys (CCHS, NPHS) • Large national questionnaire surveys • Results are representative of the Canadian population
Changes in diagnosis of hypertension in Canada Post 1999 compared to pre 1999 • Doubling of the rate of diagnosis of hypertension • Closing of the gender gap Hypertension 2006;48:853-60
Changes in the treatment of hypertension Post 1999 compared to pre 1999 • Doubling of the rate of treatment of hypertension • Closing of the gender gap Hypertension 2006;48:853-60
Changes in the proportion of thosediagnosed that are not treated Post 1999 compared to pre 1999 • Marked decrease in proportion of aware hypertensives that are untreated • Closing of the gender gap. Hypertension 2006;48:853-60
2007 Canadian Hypertension Education Program CHEP NOW HAS THE ABILITY TO IDENTIFY MANAGEMENT ISSUES • Almost 50% of women over age 60 are on drug therapy • A low proportion of younger hypertensives are on drug therapy • More than 10% of uncomplicated elderly hypertensives are started on Beta Blocker therapy.
2007 Canadian Hypertension Education Program • Canada has had continuously updated hypertension management recommendations since 1999 • A rigorous methodology is used to ensure the recommendations are reliable • An extensive implementation process is used to ensure tools are available to aid uptake of the recommendations in clinical practice • The evaluation process is still being established but preliminary data support a large increase in diagnosis and treatment of hypertension associated with a reduction in cardiovascular complications
CHEP New Initiatives • To translate the hypertension recommendations and disseminate to the public and patients with hypertension. (A partnership with Blood Pressure Canada, Canadian Hypertension Society, the Heart and Stroke Foundation and the World Hypertension League (World Hypertension Day)) • Linking to community based programs and local hypertension/ atherosclerosis clinics to facilitate the update of hypertension best management programs