Download
1 / 57
570 likes | 1.01k Views
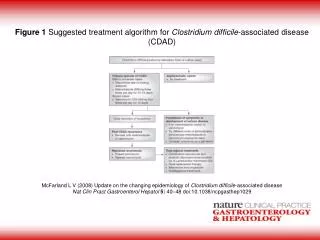
Clostridium difficile - associated disease: An update. Preeta K. Kutty, MBBS, MD, MPH Division of Healthcare Quality Promotion Centers for Disease Control and Prevention

E N D
Clostridium difficile -associated disease: An update Preeta K. Kutty, MBBS, MD, MPH Division of Healthcare Quality Promotion Centers for Disease Control and Prevention The findings and conclusions in this presentation are those of the author and do not necessarily represent the views of the Centers for Disease Control and Prevention
Overview • Background • Changing Epidemiology • Recent developments • Recommendations
Overview • Background • Changing Epidemiology • Recent developments • Recommendations
Clostridium difficle • Anaerobic spore-forming bacillus • Ubiquitous in nature • Prevalent in soil • 1935 - First described by Hall and O'Toole • Late 1970’s - Most commonly recognized cause of antimicrobial associated diarrhea - 20% -30% cases associated Hall I; O'Toole E (1935).. Am J Dis Child49: 390
Clostridium difficle :Pathogenesis • Fecal oral transmission - Reservoirs: *Contaminated environment * Hands of healthcare personnel * Hospitals & long-term care • Survive gastric acidity • Small intestine – spores germinate into vegetative forms • Large intestine – normal flora disrupted by antibiotics Diagram: Sunenshine et al Clev Clin J Med 2006 73(2) 187-197
C. difficle : Pathogenesis (contd) • C. difficile produces two toxins Toxin A – enterotoxin Toxin B – cytotoxin Enzyme immunoassay Specificity : 93 – 100% Sensitivity : 63- 99 % Diagram: Sunenshine et al Clev Clin J Med 2006 73(2) 187-197
C. difficile-Associated Disease (CDAD) • Incubation period – not known • Diarrhea – characteristic odor • Pseudomembranous colitis - First described as a complication by Larson et al in 1978 - Hallmark of CDAD - Bloody diarrhea - Raised whitish-yellow plaques - Unexplained leukocytosis (>10,000/cubic mm ) Healthy colon Pseudo-membranous colitis Larson HE et al (1978). Lancet1 (8073): 1063–1066.
Toxic megacolon • Life-threatening acute dilation • Characterized by - a dilated colon (megacolon) - Diameter : ≥ 5.5 cm - Fever, abdominal pain, abdominal distension - Radiograph: apparent edema of bowel wall • Complications : - Perforation of colon - Sepsis, Shock - Death Diagram: http://www.nlm.nih.gov/medlineplus/ency/imagepages/17189.htm
Summary: Pathogenesis of C. difficile Antibiotic therapy Disturbed colonic microflora Exposed to C. difficile Toxin A & Toxin B Diarrhea & colitis
C. difficile: Laboratory tests • Stool culture: Most sensitive - Requiring 2-3 days for growth - Unable to distinguish between the presence of toxin positive strains or toxin negative strains • Cell cytotoxin test – most specific - Cytotoxin B • Direct Enzyme immunoassay (EIA) – most frequent C difficile colonies on agar plate: http://en.wikipedia.org/wiki/Clostridium_difficile
C. difficile: Resolution and Recurrence • Resolution: 15 to 23% of patients - Within 2 to 3 days after discontinuation - But most patients require specific treatment • C. difficile diarrhea recurs after treatment in ~20% of cases • Historically mortality rate was 1 to 2.5 percent
C. difficile : Risk factors • Increasing age1 • Severe underlying gastrointestinal diseases • Exposure to Antimicrobials • Length of stay in hospital2 • Infected patients • Immune response – IgG or local IgA against toxin A3 1.Brown E et al. Infect Control Hosp Epi 1990;11: 283-90 2. Johnson S, et al Lancet 1990;336:97-100 3. M. Delmee Clin Microbiol Infect 2001; 7: 411-416
Risk factor: Antimicrobial exposure • Major risk factor for disease • Acquisition and growth of C. difficile • Suppression of normal flora of the colon • The risk doubles with longer than three days of antibiotic therapy (risk ratio: 2.28) 1 • Clindamycin, penicillins, cephalosporins • Fluroquinolones2 1.Wistrom J et al. J Antimicrob Chemother 2001;47:43-50 2. Pepin J. Clin Infect Dis. 2005 Nov 1;41(9):1254-60
Costs • Responsible for more than $1 billion annually in excess healthcare costs* - Average of $3,600 excess costs per case - Average of 3.6 extra hospital days * Kyne L, et al. Clin Infect Dis. 2002;34:346-353
Overview • Background • Changing Epidemiology • Recent developments • Recommendations
Increasing Severity of CDAD • Boston, 19981 - Very low attributable mortality • Pittsburgh, 20002 - Life-threatening disease from 1.6% to 3.2% - 44 colectomies and 20 deaths • Quebec, Canada, 20043 - Attributable mortality of 6.9% 1. Kyne L, et al. Clin Infect Dis. 2002;34:346-353 2. Dallal RM, et al. Ann Surg. 2002;235:363-372. 3. Loo VG et al.N Engl J Med. 2005 Dec 8;353(23):2442-9
National Estimates of US Short-Stay Hospital Discharges with C. difficile as First-Listed or Any Diagnosis From: McDonald LC, et al. Emerg Infect Dis. 2006;12(3):409-15
Rates of US Short-Stay Hospital Discharges with C. difficile Listed as Any Diagnosis by Age From McDonald LC, et al. Emerg Infect Dis. 2006;12(3):409-15
Overview • Background • Changing Epidemiology - Hypothesis - Facts • Recent developments • Recommendations
Hypothesis: Changein underlying host susceptibility • Increase in the average age of the population - Increase in exposure to healthcare facilities - Increase exposure to antimicrobials • However, increase in rates within small age strata that cannot be explained by aging population
Hypothesis: Use of alcohol-based hand rubs • Hand hygiene - Important prevention strategy - HCWs can transmit C. difficile • Traditional: Soap and water hand washing • Increased use of alcohol-based hand rub over the last several years
No relationship between alcohol-based hand rubs and increasing rates of CDAD Boyce et al. Infect Control Hosp Epidemiol 2006; 27:479-483
Hypothesis: Changein antimicrobial prescribing • Fluroquinolones - Popular for the management of CAP 1 - Increased use by >50% from 2000– 2002 (p<0.001)2 • Multiple antimicrobials and longer course of therapy - Greater risk3 1. Jones RN, Mandell LA. Diagn Microbiol Infect Dis. 2002;44:69–76 2. MacDougall C et al Emerg Infect Dis . 2005 ; 11(3):380-4 3. Bignardi GE. J Hosp Infect 1998; 40:1–15.
Fact : New Strain with increased virulence and resistance • Epidemic Strain - BI/NAP1 • BI - Restriction enzyme analysis (REA) group NAP1 – North American PFGE type 1 • Resistant to fluroquinolones
2 1 2 1 1 1 Acute Care Hospitals with CDAD Outbreaks* Between 2001-2004 *Detected by increases in the number of positive routine clinical laboratory tests for C. difficile. Data from McDonald LC, et al. N Engl J Med. 2005;353:2433-2441.
Increased Toxin A Production invitro In vitro production of toxins A and B by C. difficile isolates. Median concentration and IQRs are shown. C. difficile strains included 25 toxinotype 0 and 15 NAP1/027 strains (toxinotype III) from various locations. Warny M, et al. Lancet. 2005;366:1079-1084.
Increased Toxin B Production in vitro In vitro production of toxins A and B by C. difficile isolates. Median concentration and IQRs are shown. C. difficile strains included 25 toxinotype 0 and 15 NAP1/027 strains (toxinotype III) from various locations. From Warny M, et al. Lancet. 2005;366:1079-1084.
States with the Epidemic Strain of C. difficile (N=23),Updated 10/11/2006 DC HI PR AK
Challenges • Emergence of a new epidemic strain - Increased resistance to fluoroquinolones - Responsible for at least some increase in cases and severity
Overview • Background • Changing Epidemiology • Recent developments • Recommendations
Severe CDAD in Populations Previously at Low Risk—Four States, 2005 • Recent reports to the Pennsylvania Department of Health and CDC May –June 2005 (33 cases) • 23 Young patients without serious underlying disease • C.difficile toxin-positive by routine diagnostic testing • Responded to CDAD-specific therapy • Peripartum - 10 patients • Within 4 weeks of delivery • Reports from PA, NJ, OH, and NH CDC. MMWR. 2005;54:1201-1205.
Severe CDAD in Populations Previously at Low Risk—Four States, 2005 (contd) • Community-associated (CA-CDAD) • No hospital exposure in prior 3 months • Reports from Philadelphia and 4 surrounding counties • 8 (24%) had no exposure to anti-microbial agents within 3 months before CDAD onset. • 10 (30%) had received clindamycin CDC. MMWR. 2005;54:1201-1205.
Investigation of CA-CDAD in North Carolina, 2005* • Study period : Jan 1st - Dec 31st, 2005 • Six hospitals – Four Veterans Affairs - One Regional - One University * Kutty et al - CDC , unpublished data
Investigation of CA-CDAD in North Carolina, 2005 (contd) • Definitions CDAD : Diarrhea in a patient with a positive C. difficile toxin assay. Community Associated (CA) CDAD : CDAD onset in the community or within 72 hours of hospital admission, in a patient and No inpatient healthcare exposure within the previous 2 months. Kutty et al - CDC , unpublished data
Investigation of CA-CDAD in North Carolina, 2005 (contd) Kutty P, et al - CDC , unpublished data • 1,100 CDAD cases • To date: • - 209 (19%) identified as CA CDAD • (range 15-47% per hospital) • - Substantial proportion of CDAD • Case control (1 to 2 ) study at 4 VA hospitals • Ongoing study
VA case control study Demographics Kutty P, et al - CDC , unpublished data
VA case control study Predisposing factors Kutty P, et al - CDC , unpublished data
VA case control study Multivariable analysis Kutty P, et al - CDC , unpublished data
Overview • Epidemiology • Changing Epidemiology • Recent developments • Recommendations
Overview • Epidemiology • Changing Epidemiology • Recent developments • Recommendations -Hospitals
Recommendations for Hospitals • Hospitals should conduct surveillance for CDAD • Track positive laboratory results (eg, toxin A or A/B assays) • Consider measures to track outcomes • Early diagnosis and treatment important for reducing severe outcomes and should be emphasized
Recommendations for Hospitals(contd.) Strict infection control 1 • An environmental cleaning and disinfection strategy • Prevent Transmission (Step 11 &12)2 - Contact precautions for CDAD patients - Hand-washing in outbreak • CDC C. difficile Fact Sheets: http://www.cdc.gov/ncidod/dhqp/. • Campaign: http://www.cdc.gov/drugresistance/healthcare/
HICPAC and Hand Hygiene Task Force: Hand Hygiene Washing hands with non-antimicrobial or antimicrobial soap and water may help to physically remove spores from the surface of contaminated hands. HCWs should be encouraged to wear gloves when caring for patients with C. difficile associated diarrhea. After gloves are removed, hands should be washed with a non- antimicrobial or an antimicrobial soap and water or disinfected with an alcohol based hand rub. http://www.cdc.gov/mmwr/PDF/rr/rr5116.pdf
CDC Guidelines: Hand Hygiene During outbreaks of C. difficile-related Infections, washing hands with a non- antimicrobial or antimicrobial soap and water after removing gloves is prudent. http://www.cdc.gov/mmwr/PDF/rr/rr5116.pdf
Recommendations for Hospitals(contd.) Use Antimicrobials Wisely * • Step 5. Practice antimicrobial control -Engage in local antimicrobial control efforts • Step 6. Use local data -Know your antibiogram. -Know your patient population • Step 7 and 8. Treat infection, not contamination and colonization -Use proper antisepsis for blood and other cultures. -Use proper methods to obtain and process all cultures. *Campaign: http://www.cdc.gov/drugresistance/healthcare/
Recommendations for Hospitals (contd.) Use Antimicrobials Wisely • Step 10. Stop antimicrobial treatment:- When infection is cured - When cultures are negative and infection is unlikely - When infection is not diagnosed • Further research needed • Role for specific antimicrobial controls in stemming this epidemic
Overview • Epidemiology • Changing Epidemiology • Recent developments • Recommendations - Hospitals - Previously Low-Risk Populations
Recommendations for CDAD in Previously Low-Risk Populations Previously Low-Risk Populations • Further investigation and surveillance in these populations are warranted • Strains responsible for severe CDAD in previously low-risk populations unknown • May be other toxin variants and/or hospital epidemic strain • Clinicians should consider the diagnosis - CDAD in patients without traditional risk factors
Recommendations for CDAD in Previously Low-Risk Populations (contd) • Patients should seek medical attention • Diarrhea lasting longer than 3 days • Fever • Blood • Antimicrobial exposure is not benign • Continue to emphasize judicious antimicrobial use
You can help • Efforts are needed to improve adherence to recommendations for infection control and antimicrobial use • CDC’s Campaign to Prevent Antimicrobial Resistance in healthcare settings can serve as a framework to motivate clinicians