Download

1 / 25
320 likes | 821 Views
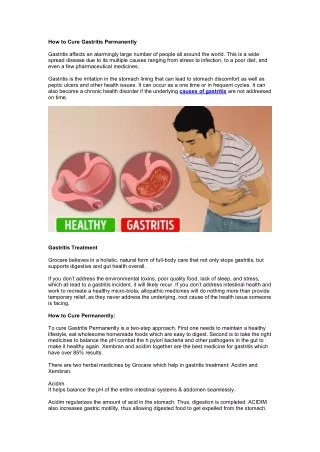
GASTRITIS. Definition: Inflammation of the gastric mucosa group of disorders with inflammatory changes in the gastric mucosa (G.M.) that have different clinical features, histological characteristics and pathogenesis. A. ACUTE GASTRITIS B. CHRONIC GASTRITIS.

E N D
Definition: Inflammation of the gastric mucosa • group of disorders with inflammatory changes in the gastric mucosa (G.M.) that have different clinical features, histological characteristics and pathogenesis. • A. ACUTE GASTRITIS • B. CHRONIC GASTRITIS
A. ACUTE HEMORAGIC GASTRITIS (EROSIVE) Examinationshows: EDEMA MUCOSAL FRIABILITY EROSIONS: limited to the mucosa ! SITES OF BLEEDING: diffusely through the G. M. localized to the body, antrum of the stomach HISTOLOGIC EXAMINATIONof the G.M. reveals infiltration of the lamina propria with: – mononuclear cells – PMN leukocytes – extravasations of blood in the mucosa
ETIOLOGY & PATHOGENESIS: Erosive gastritis – 89 - 90 % of critically ill hospitalized patients (medical) surgical intensive care units Stress – induced gastritis Mechanism: a) ischemia of the G.M. b) acid diffusion from the gastric lumen into gastric mucosal tissues c) bile acid / duodenal pancreatic secretions refluxed into the gastric lumen a + b CRUCIAL in the ethiopathogenesis of the STRESS – INDUCED GASTRITIS AGENTS injure the G.M. - aspirin – injure the small vessels in the G.M. by: –inhibitory of prostacyclin in the walls of vessels –synthesis of tromboxane by platelets - NSAIDS - bile acids - pancreatic enzymes - ethanol Reduction in tissue PG – principal in damage the G.M.
CLINICAL FEATURES PHYSICAL EXAMINATION • Hematemesis / melena Pallor • Anemia Tachycardia • Epigastric pain Hypotension • Nausea • Vomiting • BIOLOGICAL ASPECTS • - leucocytosis / leukopenia
DIAGNOSIS • blood in the stool / gastric aspirate • Upper GI endoscopy: • mucosal hemorrhages • friability + congestion • erosions • superficial / deep ulcerations in the fundus / body of the stomach • Radiographic examination – much less reliable in detecting acute hemoragic erosive gastritis • TREATMENT • A. General supportive measures • - maintenance of oxygen, blood volume, fluid and electrolyte requirements • B. H2 – R antagonist (i.v.) QUAMATEL 20 – 40 mg/day • Embolization / vasopressin infusion of the left gastric artery • IPP – Controloc 40 mg i.v. • Surgical treatment should not be performed unless is absolutely necessary.
ACUTE GASTRITIS + HELICOBACTER PYLORI - short spiral – shaped, microaerophitic gram - bacillus - in gastric samples by histological examination, culture, increase activity, by endonuclease analysis. - hematoxylin – positive - UBT 13C, 14C - antibodies (Ig G, Ig A) to H.P. 90 – 100 % Hp + antral biopsy specimens of DU patients 70 % - G.U. 80 % - chronic gastritis involving the antral mucosa 50 % - non ulcer dyspepsia
CHRONIC GASTRITIS Definition: Chronic inflammatory cells, predominately lymphocytes and plasma cells. HISTOLOGIC CLASSIFICATION I. SUPERFICIAL GASTRITIS - Inflammatory changes in the lamina propia of the superficial mucosa of the upper half of G.M. and the glands are preserved II. ATROPHIC GASTRITIS - the inflammatory infiltrate extends to the deep positions of the mucosa - profound loss of the glandular structures which are separated widely by connective tissue, with a greatly reduced / absent inflammatory infiltrate. - the mucosa is thin, revealing the prominence of its underlying vessels by endoscope examination. Gastritis progresses – changes in the morphology of the gastric glandular elements. Intestinal metaplasia – conversion of gastric glands to the small-intestinal mucosal glands with goblet cells.
CHRONIC GASTRITIS – TYPES A & B Type A – involves the body and fundus of the stomach – from that may lead to pernicious anemia Antibodies to parietal cells, intrinsec factor in serum immuno / autoimmuno pathogenesis Parietal cell Antibodies 20% of patients over age 60 20% of patients with – hypoparathyroidism – Addison’s disease – vitiligo Antibodies to intrinsec factor 40 % of those with pernicious anemia. The risk of stomach cancer in patients with type A gastritis and pernicious anemia is three times than the general population Type B: In younger patients involves the antrum In elderly patients involves entire stomach The incidence increases with age - Strong associations of H. pylori with type B gastrities - Chronic reflux of: pancreatic – biliary secretions bile acids lysolecithin
DIAGNOSIS • - Biopsy of the G.M. provides the most reliable means of identifying and classifying gastritis. • Several biopsies of suspected areas, when safe and possible, are recommended. • TREATMENT • In type A.G. + pernicious anemia • Vit. B12 – indefinite regular parental administration
MÉNÉTRIER’S DISEASE • - large tortuoces gastric mucosal folds in gastric body and fundus. • - hyperplasia of surface and glandular mucous cells, which replace most of the chief and parietal cells. • the lamina propria may contain an increased number of lymphocytes and intestinal metaplasia may be present. • Symptoms • epigastric pain • anorexia • nausea, vomiting • weight loss • gastric bleeding – unusual Gastric ulcer / gastric carcinoma many develop ! • Gastric acid secretion is reduced / absent. • Barium examination: large gastric folds • Endoscopic examination: confirm gastric folds • Diagnostic: deep mucosal biopsy • Treatment:ARH2 decrease protein loss • high – protein diet to replace protein loses • gastrectomy in severe disease
CORROSIVE GASTRITIS - corrosive chemicals antrum injury (HCl, H2SO4, NaOH) Symtoms: burning of the mouth, throat, retrosternal area epigastric pain vomiting hemorrhage / perforation Treatment: supportive therapy
INFECTIOUS GASTRITIS Phlegmonous G – necrosis, sepsis - streptococci, staphylococci, Proteus, Escherichia coli TREATMENTi.v. antibiotics fluids + electrolyte replacement gastrectomy – in lack of response It can occur in immuno-compromised patients cytomegalovirus
EOSINOPHILIC GASTRITIS • extensive eosinophilic infiltration (e.i) of the wall of the stomach • -biopsy reveals e.i. • - antrum is more frequently involved than G body fundus. • SYMPTOMS: epigastric pain • nausea, vomiting • TREATMENT:glucocorticoids
GRANULOMATOUS GASTRITIS Chron’s disease produce: ulceration granulomatous infiltration stricture formation Other’s: histoplasmosis candidosis syphilis tuberculoses Diagnostic: biopsies + cytology to exclude malignancy surgical exploration if the diagnostic is not established by biopsy at endoscopy.
DUODENAL ULCER Chronic and recurrent disease ETIOLOGY - Genetic Factors: increase of blood 0 - increase HLA – B5 antigen in white male subjects - 50 % - elevated serum pepsinogen (PG I) - autosomal dominant trait - Smoking – inhibition of pancreatic bicarbonate secretion by nicotine – accelerated emptying of gastric acid into the duodenum - Chronic renal failure - Alcoholic cirrhosis - Gastric colonization with Helicobacter pylori in 80 -100% - Psychological factors: chronic anxiety, stress
CLINICAL FEATURES 1. Epigastric pain: sharp, burning, gnawing 10 % - right epigastrium 2. Occurs from 90’ - 3 hours after eating awakens the patients at night - pain is usually relieved by food or antacids - nausea, vomiting - weight loss - anemia (occult blood loss) – iron deficiency - constipation - Penetration - Perforation 6% / complications - Hemorrhage: 15% with 40 % reccurence
DIAGNOSIS 1. Barium examinationUGIT 70 – 80 % + discrete crater in the proximal portion of the duodenal bulb 2. Endoscopic examination
MEDICAL TREATMENT 1. Antacids:Aluminum hydroxide Magnesium Calcium carbonate Sodium bicarbonate 2. H2 – R antagonists Cimetidine 300 mg x 4 / days 4 weeks Adverse effects: increase transaminase, creatinine, gynecomastia Ranitidine: 150 mg x 2 / day 300 mg at bedtime Nizatidine:300 mg 1 month 150 mg bedtime for reduction of DU recurrence Famotidina: 20 – 40 mg / day 4 weeks 3. Anticholinergic agents:atropine decrease gastric acid secretion (g.a.s.) Pirenzepine – adjunctive therapy
4. Coating agents Sucralfate increase mucosal defense! Colloidal bismuth 5. Prostaglandinsreduce basal and stimulated g.a.s. enhances mucosal resistance to tissue injury. 6. Proton Pomp Inhibition - OMEPRAZOLE 20 mg X 2 / DAY 4 – 6 weeks - LANSOPRAZOLE 30 mg / day - PANTOPRAZOLE 40 mg / day - ESOMEPRAZOLE 20 – 40 mg / day DIET - free of spices, fruit juices - avoid coffee, alcohol intake - elimination of smoking - elimination stress eat 5 times / day in small meals
GASTRIC ULCER (G.U.) • the pick incidence for G.U. is in the sixth decade • ETIOLOGY • Acid- pepsin appears important in the pathogenesis • - Gastric emptying is delayed • Regurgitation of duodenal contents (bile) induce gastric mucosal injury- gastric ulceration • CLINICAL FEATURES • - Epigastric pain - no relief with eating! • - Nausea, vomiting • - Weight loss • - Upper GI bleeding • - Anemia
DIAGNOSIS • 1. Barium examination • 2. Endoscopy: size, location, histological characteristics • Ulcer > 3 cm diameter are > often malignant • 4% of GU appears benign on X-Ray plane to be malignant by endoscopic biopsy / surgery! • MEDICAL TREATMENT • H2RA • Sulcralfate 4/ 8 weeks • Antacids • Benign G.U. should heal completely within 3 months of vigorous therapy. • Avoid - NSAID/ glucocorticoides • - coffee • - smoking • - spices foods • Gastroscopy after 4 weeks of treatment reveal healing of benign ulcers.
Surgery in D.U. • - Vagotomy + antrectomy • - vagotomy + pyloroplasty • - truncal or selective vagotomy • - Bilroth IA: stomach + proximal duodenum • Bilroth IIA: stomach + loop of the jejunum • Surgery GU: Antrectomy + G.D. Anastomosis in those who do not respond to medical theraphy/complications. • GASTRIC ADENOCARCINOMA • 90% are adenocarcinomas • 10% non// Hodgkin's lymphomas and leiomyosarcomas.
ETIOLOGY • Long/term ingestion of high concentrations of nitrates indried, smoked, salted foods- higher risk. Serial endoscopic examination of the stomach in patients with atrophic gastritis- replacement of the gastric mucosa by intestinal type cells/ cellular atypia/ neoplasia • - Adenomatous polyposis • - Gastric ulcers • - Menetrier's disease • Group AII patients • CLINICAL FEATURES • - Upper abdominal discomfort- steady pain • - Anorexia • - Weight loss • - Nausea + vomiting - tumor of the pylorus • - Disphagya - tumor of cardia • - Palpable abdomen mass-physic examination • - Iron - deficiency anemia • - Migratory thrombophlebitis • - microangiopathie hemolytic anemia • - Achantosis nigricans.
DIAGNOSIS • Double-contrast radiographic examination. • Deep Gastroscopic biopsy and brush cytology. • TREATMENT • Surgical removal of the complete T, with resection of adjacent lymph nodes offers the only chance for cure. • Subtotal gastrectomy - distal carcinomas. • Total gastrectomy - proximal tumors. • PROGNOSIS • - degree of tumor penetration into the stomach wall. • - regional lymph node involement/ vascular invasion. • Chemotherapy and/or radiotherapy - metastatic disease (5 FU+ Doxorubicin, Mytomicin + G cisplatin) • PRIMARY GASTRIC LYMPHOMA • 7% of gastric malignancies/ 2% of all lymphomas. • GASTRIC SARCOMA • - 1-3% of all gastric neoplasms • - anterior + posterior walls of the gastric fundus • - spread to the liver and lungs.