Download
1 / 24
540 likes | 2.01k Views
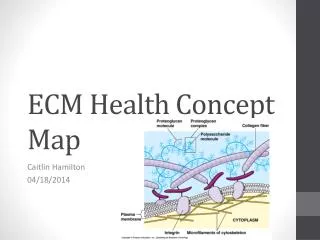
EXTRACELLULAR MATRIX (ECM) AND CELL-MATRIX INTERACTIONS. The ECM is a dynamic, constantly remodeling macromolecular complex synthesized locally, which assembles into a network that surrounds cells. It constitutes a significant proportion of any tissue.

E N D
EXTRACELLULAR MATRIX (ECM) AND CELL-MATRIX INTERACTIONS • The ECM is a dynamic, constantly remodeling macromolecular complex synthesized locally, which assembles into a network that surrounds cells. • It constitutes a significant proportion of any tissue. • ECM is important for cell adhesion and serve as a reservoir for growth factors, thus, ECM regulates the proliferation, movement, and differentiation of the cells living within it. • Synthesis and degradation of ECM accompanies morphogenesis, wound healing, chronic fibrotic processes, and tumor invasion and metastasis
ECM • ECM occurs in two basic forms: interstitial matrix and basement membrane 1- Interstitial Matrix: • present in the spaces between cells in connective tissue; • it is synthesized by mesenchymal cells (e.g., fibroblasts) • and tends to form a three-dimensional, amorphous gel. • Its major constituents are fibrillar and nonfibrillar collagens, as well as fibronectin, elastin, proteoglycans, hyaluronate, and other elements
ECM 2- The basement membrane: • lies beneath the epithelium • is synthesized by overlying epithelium and underlying mesenchymal cells • Its major constituents are amorphous nonfibrillar type IV collagen and laminin
ECM functions 1- Mechanical support for cell anchorage and cell migration 2-maintenance of cell polarity 3- Control of cell growth 4- Maintenance of cell differentiation 5- Scaffolding for tissue renewal. 6- Establishment of tissue microenvironments. 7- Storage and presentation of regulatory molecules: FGF and HGF are excreted and stored in the ECM. This allows the rapid deployment of growth factors after local injury • Although labile and stable cells are capable of regeneration, injury to these tissues results in restitution of the normal structure only if the ECM is not damaged. Disruption of these structures leads to collagen deposition and scar formation.
Components of ECM • There are three basic components of ECM: (1) fibrous structural proteins such as collagens and elastins, which confer tensile strength and recoil (2) water-hydrated gels such as proteoglycans and hyaluronan, which permit resilience and lubrication (3) adhesive glycoproteins that connect the matrix elements to one another and to cells
Collagens • are fibrous structural proteins that confer tensile strength. • are composed of three separate polypeptide chains braided into a ropelike triple helix. • About 30 collagen types have been identified • Some collagen types (e.g., types I, II, III, and V) form fibrils by virtue of lateral cross-linking of the triple helices. These are called the fibrillarcollagens, and form a major proportion of the connective tissue in healing wounds and particularly in scars • Other collagens are nonfibrillar and present in basement membrane (type IV) • The tensile strength of the fibrillar collagens derives from their cross-linking, which is the result of covalent bonds. This process is dependent on vitamin C; therefore, children with vitamin C deficiencyhave skeletal deformities, bleed easily because of weak vascular wall basement membrane, and heal poorly
Elastin • the ability of tissues to recoil and return to a baseline structure after physical stress is conferred by elastic tissue. • This is especially important in the walls of: vessels , the uterus, skin, and ligaments.
Proteoglycans and Hyaluronan • Proteoglycans form highly hydrated compressible gels conferring resilience and lubrication (such as in the cartilage in joints). • They consist of long polysaccharides called glycosaminoglycans (examples are dermatan sulfate and heparan sulfate) linked to a protein backbone. • Hyaluronan a huge molecule composed of many disaccharide repeats without a protein core, is also an important constituent of the ECM. Because of its ability to bind water, it forms a viscous, gelatin-like matrix
Adhesive glycoproteins and adhesion receptors • are structurally diverse molecules involved in cell-to-cell adhesion, the linkage between cells and ECM, and binding between ECM components. • The adhesive glycoproteins include fibronectin (major component of the interstitial ECM) and laminin (major constituent of basement membrane). • The adhesion receptors, also known as cell adhesion molecules (CAMs), are grouped into four families: immunoglobulins, cadherins, selectins, and integrins
Fibronectin • is a large disulfide-linked heterodimer • synthesized by a variety of cells, including fibroblasts, monocytes, and endothelium. • Fibronectinscan bind to a wide spectrum of ECM components (e.g., collagen, fibrin, heparin, and proteoglycans) and can also attach to cell integrins. • Fibronectin mRNA has two splice forms, which generate: 1- tissuefibronectinformsfibrillar aggregates at wound healing sites 2- plasmafibronectin binds to fibrin to form the provisional blood clot of a wound, which serves as a base for ECM deposition and re-epithelialization
Laminin • is the most abundant glycoprotein in basement membrane. • connects cells to underlying ECM components such as type IV collagen and heparan sulfate, mediating attachment to basement membrane. • laminin can also modulate cell proliferation, differentiation, and motility.
REPAIR BY CONNECTIVE TISSUE • Repair begins within 24 hours of injury by the emigration of fibroblasts and the induction of fibroblast and endothelial cell proliferation. • By 3 to 5 days, a specialized type of tissue that is characteristic of healing, called granulation tissue, is apparent. • The term granulation tissue derives from the pink, soft, granular gross appearance, such as that seen beneath the scab of a skin wound. • Microscopically proliferation of fibroblasts and new thin-walled, delicate capillaries (angiogenesis), in a loose ECM
Granulation tissue then progressively accumulates connective tissue matrix, eventually resulting in the formation of a scar, which may remodel over time
Mature scar tissue Granulation tissue Note: Blue represents collagen fibers stained by trichrome stain
REPAIR BY CONNECTIVE TISSUE • Repair by connective tissue deposition consists of four sequential processes: • 1-Formation of new blood vessels (angiogenesis) • 2-Migration and proliferation of fibroblasts • 3-Deposition of ECM (scarformation) • 4-Maturation and reorganization of the fibrous tissue (remodeling)
Angiogenesis • The main steps that occur in angiogenesis from preexisting vessels are listed below: 1- Vasodilation in response to NO and increased permeability of the preexisting vessel induced by vascular endothelial growth factor (VEGF) 2- Migration of endothelial cells toward the area of tissue injury 3- Proliferation of endothelial cells 4- Inhibition of endothelial cell proliferation and remodelinginto capillary tubes 5- Recruitment of periendothelial cells (pericytes for small capillaries and smooth muscle cells for larger vessels) to form the mature vessel
Angiogenesis • New vessels formed during angiogenesis are leaky (incompletely formed interendothelial junctions and VEGF increases vessel permeability). This explains why granulation tissue is often edematous. • Growth Factors Involved in Angiogenesis: Several factors induce angiogenesis, but the most important are VEGF and basic fibroblast growth factor (FGF-2).
VEGF • VEGFs are dimericglycoproteins with many isoforms • Several agents can induce VEGFs, the most important being hypoxia. Other inducers are platelet-derived growth factor (PDGF), TGF-β, and TGF-α
FGFs • constitute a family of factors with more than 20 members, the best characterized are FGF-1 (acidic FGF) and FGF-2 (basic FGF). • are produced by many cell types • FGF-2 participates in angiogenesis mostly by stimulating the proliferation of endothelial cells. • It also promotes the migration of macrophages and fibroblasts to the damaged area, and stimulates epithelial cell migration to cover epidermal wounds.
Migration of Fibroblasts and ECM Deposition (Scar Formation) • It builds on the granulation tissue framework of new vessels and loose ECM that develop early at the repair site. • It occurs in two steps: • migration and proliferation of fibroblasts into the site of injury • deposition of ECM by these cells • The recruitment and stimulation of fibroblasts is driven by many growth factors, including PDGF, FGF-2, and TGF-β.
As healing progresses: • the number of proliferating fibroblasts and new vessels decreases • increased deposition of ECM. • Increased collagen synthesis (strength) • collagen synthesis by fibroblasts begins early in wound healing (days 3 to 5) and continues for several weeks, depending on the size of the wound • granulation tissue scaffold evolves into a scar (composed of spindle-shaped fibroblasts, dense collagen, fragments of elastic tissue, and other ECM components) • vascular regression (the highly vascularized granulation tissue transforms into a pale avascular scar)
Growth Factors Involved in ECM Deposition and Scar Formation • Many growth factors are involved in these processes, including TGF-β, PDGF, and FGF • TGF-β: • belongs to a family of homologous polypeptides • has many and often opposite effects, depending on the cell type and the metabolic state of the tissue. • In the context of inflammation and repair, TGF-β has two main functions:
TGF-β functions 1- is a potent fibrogenic agent. • It stimulates the production of collagen, fibronectin, and proteoglycans • It inhibits collagen degradation by both decreasing proteinase activity and increasing the activity of tissue inhibitors of proteinases known as TIMPs . • TGF-β is involved not only in scar formation after injury but also in the development of fibrosis in lung, liver, and kidneys that follows chronic inflammation. 2-TGF-β inhibits lymphocyte proliferation and can have a strong anti-inflammatory effect.