MRSA: Implications in Sports Medicine
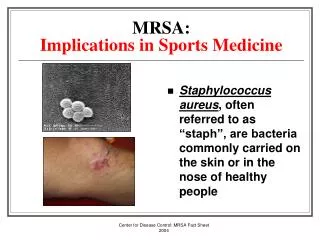
MRSA: Implications in Sports Medicine Staphylococcus aureus , often referred to as “staph”, are bacteria commonly carried on the skin or in the nose of healthy people Staphylococcus Aureus Occasionally, staph can cause an infection

MRSA: Implications in Sports Medicine
E N D
Presentation Transcript
MRSA:Implications in Sports Medicine • Staphylococcus aureus, often referred to as “staph”, are bacteria commonly carried on the skin or in the nose of healthy people Center for Disease Control: MRSA Fact Sheet 2004
Staphylococcus Aureus • Occasionally, staph can cause an infection • Staph bacteria are one of the most common causes of skin infections in the US • Most of these infections are minor • pimples, boils • Most can be treated without antibiotics • However, staph infections can cause serious infections • surgical wound infections, pneumonia Center for Disease Control: MRSA Fact Sheet 2004
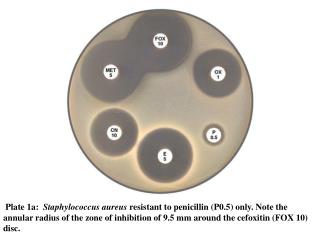
MRSA:Methicillin-Resistant Staphylococcus Aureus • In past, most serious staph bacterial infections were treated with a certain type of antibiotic related to penicillin • In recent years, treatment of these infections more difficult because staph bacteria have become resistant to various antibiotics, including the commonly used penicillin related antibiotics • These resistant bacteria are called methicillin-resistant staphylococcus aureus, or MRSA Center for Disease Control: MRSA Fact Sheet 2004
Where are staph and MRSA found ? • Staph bacteria and MRSA can be found on the skin and in the nose of some people without causing illness. Center for Disease Control: MRSA Fact Sheet 2004
What is the difference between colonization and infection ? • Colonization occurs when the staph bacteria are present on or in the body without causing illnesss • ~25-30% of the population is colonized in the nose with staph bacteria at a given time Center for Disease Control: MRSA Fact Sheet 2004
What is the difference between colonization and infection ? • Infection occurs when the staph bacteria cause disease in the person • People also may be colonized or infected with MRSA, the staph bacteria that are resistant to many antibiotics Center for Disease Control: MRSA Fact Sheet 2004
Who gets MRSA ? • Staph bacteria can cause different types of illness • skin infections, bone infections, pneumonia, severe life-threatening bloodstream infections, and other illnesses • Since MRSA is a staph bacterium, it can cause the same types of infections as staph in general; however, MRSA occurs more commonly among persons in hospitals and healthcare facilities Center for Disease Control: MRSA Fact Sheet 2004
Who gets MRSA ? • MRSA infection usually develops in hospitalized patients: • elderly • very sick • open wound • tube going into body • IV or catheter • MRSA infections acquired in hospitals and healthcare settings can be severe Center for Disease Control: MRSA Fact Sheet 2004
Who gets MRSA ? • Certain factors can put some patients at higher risk for MRSA: • prolonged hospital stay • receiving broad-spectrum antibiotics • being hospitalized in an intensive care or burn unit • spending time close to other patients with MRSA • recent surgery • carrying MRSA in nose without developing illness Center for Disease Control: MRSA Fact Sheet 2004
Who gets MRSA ? • MRSA causes illnesses in persons outside of hospitals and healthcare facilities as well • Cases of MRSA diseases in the community have been associated with: • Injecting drug users • Aboriginals in Canada, New Zealand or Australia • Native Americans in US • Incarcerated persons • Players of close contact sports Center for Disease Control: MRSA Fact Sheet 2004
Community-Associated MRSA • Community-associated MRSA infections are typically skin lesions, but can also cause severe illness • Most of transmissions appear to be from people with active MRSA skin infections Center for Disease Control: MRSA Fact Sheet 2004
How common is staph and MRSA ? • Staph bacteria are one of the most common causes of skin infection in the US and are a common cause of pneumonia and bloodstream infections • Staph and MRSA infections are not routinely reported to public health authorities, so a precise number is not known • Estimated as many as 100,000 persons are hospitalized each year with MRSA infections • only small proportion of these have disease onset occuring in the community Center for Disease Control: MRSA Fact Sheet 2004
How common is staph and MRSA ? • ~ 25-30% of the population is colonized in the nose with staph bacteria at a given time • Numbers who are colonized with MRSA at any one time is not known • CDC is currently collaborating with state and local health departments to improve surveillance for MRSA Center for Disease Control: MRSA Fact Sheet 2004
Are staph and MRSA infections treatable ? • Yes. Most staph bacteria and MRSA are susceptible to several antibiotics • Furthermore, most staph skin infections can be treated without antibiotics by draining the sore • However, if antibiotics are prescribed, patients should complete the full course and consult their physicians if the infection does not get better Center for Disease Control: MRSA Fact Sheet 2004
How are staph and MRSA spread ? • Staph bacteria and MRSA can spread among people having close contact with infected people • MRSA is almost always spread by direct physical contact, and not through the air • Spread may also occur through indirect contact by touching objects contaminated by the infected skin of a person with MRSA or staph bacteria • towels, sheets, wound dressings, clothes, workout areas, sports equipment Center for Disease Control: MRSA Fact Sheet 2004
How can I prevent staph orMRSA infections? • Practice Good Hygiene !!! • Keep your hands clean by washing thoroughly with soap and water • Keep cuts and abrasions clean and covered with a proper dressing until healed • Avoid contact with other people’s wounds or material contaminated from wounds Center for Disease Control: MRSA Fact Sheet 2004
Management of Staph or MRSA Infections in Athletic Setting • Cover all wounds • if wound cannot be covered adequately, consider excluding players with potentially infectious skin lesions from practice and/or competition until lesions are healed or can be covered adequately • Encourage good hygiene, including showering and washing with soap after all practices and competitions • Ensure availability of adequate soap and hot water • pump soap dispensers with antibacterial soap; no bar soap Center for Disease Control: MRSA Fact Sheet 2004
Management of Staph or MRSA Infections in Athletic Setting • Discourage sharing of towels and personal items • clothing or equipment • Establish routine cleaning schedules for shared equipment • Train athletes and coaches in first aid for wounds and recognition of wounds that are potentially infected • Encourage athletes to report skin lesions to sports medicine staff • Encourage coaches and sports medicine staff to assess regularly for skin lesions Center for Disease Control: MRSA Fact Sheet 2004
What should I do if I think one of my student-athletes has a staph or MRSA infection ? • Consult your team physician !!! Center for Disease Control: MRSA Fact Sheet 2004
Treatment of MRSA Infection • Incision and drainage • Culture wound • Pharmacologic/supportive treatment • Minocycline 100 mg po bid x 14 days (Septra DS as alternative) • Rifampin 600 mg po qday x 14 days • Bactroban: apply to nares bid x 14 days • Hibiclens: head to toe bath • Wash all bedding/clothes in dilute bleach solution • Unresponsive patients • Vancomycin IV; Zyvox (linezolid), Cubicin (Daptomycin) IV Center for Disease Control: MRSA Fact Sheet 2004
References 1. CDC. Methicillin-Resistant Staphylococcus aureus infections among competitive sports participants --- Colorado, Indiana, Pennsylvania, and Los Angeles County, 2000—2003. MMWR 2003; 52(33); 793-795. 2. http://dermis.multimedica.de/doia 3. http://dermnetnz.org/bacterial/boils.html 4. www.cubicin.com 5.www.eurekalert.org/pub_releases/2004-10/epr-dsz100104.php Center for Disease Control: MRSA Fact Sheet 2004