Download
1 / 32
320 likes | 1k Views
Double Switch Operation for Failing Systemic Ventricle. Yong Jin Kim, M.D. Department of Thoracic & Cardiovascular Surgery Seoul National University Hospital. Introduction.

E N D
Double Switch Operation for Failing Systemic Ventricle Yong Jin Kim, M.D. Department of Thoracic & Cardiovascular Surgery Seoul National University Hospital 2001.7
Introduction • Conventional managements of AV discordant heart ( Atrial switch operation in TGA) place morphologic right ventricle & tricuspid valve in the systemic position • The morphologic RV shows significant incidence of progressive ventricular dysfunction & TV regurgitation • Double switch operation(conversion switch operation) as an alternative in selected patients 2001.7
Natural History of CC-TGA • 1. Incidence 0.5% of CHD, slightly male predominating • 2. Heart Block • 1) Complete heart block • 5 - 10% at birth. 10 - 15% in adolescence, 30% in adult • 2) 1st or 2nd degree A-V block ; 40 - 50% at birth • 3) 40% retain normal PR interval & QRS through their lives • 3. Ventricular function Not truly normal, but sufficiently good in most • Tendency to deteriorate after 2nd –3rd decade of life. • 4. Effect of coexisting cardiac anomalies • VSD, PS, left A-V valve incompetence 2001.7
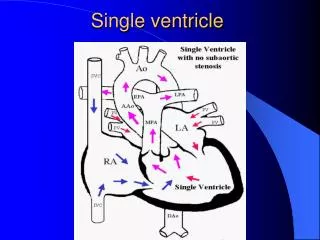
Characteristics of Both Ventricles 1. Ventricle Shape • Cylindric vs. crescent-shaped cavity 2. Contraction pattern • Concentric vs. bellow-like contraction 3. Pumping action • Pressure pump vs. low pressure-volume pump • Its large internal surface area-to-volume ratio 4. Coronary artery supply • Two system vs. one system 5. Embryology • Primitive ventricle vs. bulbus cordis 6. Papillary muscles • Two papillary vs. small and numerous(septophylic) 2001.7
Corrected TGA 2001.7
Corrected TGA 2001.7
Operative Indications of CC-TGA • The presence of corrected TGA is not an indication • for a reparative operation • 1. Ventricular septal defect · same as normal heart • 2. VSD & Important PS • · same as TOF • 3. Left-sided tricuspid incompetence • · same as mitral incompetence • 4. Complete heart block 2001.7
Classic Operation of CC-TGA • 1. Repair of ventricular septal defect • 2. Repair of coexisting VSD & PS • · Extracardiac conduit • · Without extracardiac conduit • 3. Correction of incompetent tricuspid valve • · Repair ( annuloplasty ) • · Replacement • 4. Fontan-type repair • Straddling, A-V canal defect& hypoplastic • ventricle 2001.7
“ Classic” Repair of Congenitally Corrected TGA and VSD(Termignon JL, et al. Ann Thorac Surg 1996) • From 1974 to 1994, 52 CCTGA patients • CCTGA and VSD + LVOTO(Group I) : 37 • CCTGA and Isolated VSD(Group II) : 15 • Tricuspid plasty or replacement • 1 (3%) in group I, 8 (53%) in group II • Overall operative mortality : 15% (8/52) • Incidence of postop. AV block 27% (14/52) • Redo tricuspid plasty or replacement in 12 • The operative mortality and the incidences of TVR & AV block are high • Secondary heart failure is frequent 2001.7
Tricuspid Regurgitation & RV dysfunction in CC-TGA • High risk of TR development by the 3rd decade of life(20 to 50%) • Most important risk factor for death after classic repairs • Poorly supported tricuspid annulus – RV dysfunction may induce important TR • Measurable deterioration of RV within 3 years of classic repairs • RV dysfunction appears to be almost always secondary to long-standing TR(Prieto, et al. Circulation.1998) 2001.7
Morphologic RV after Atrial Switch Operation • Natural difference of ventricle • One coronary ventricle • One conduction radiation • Without well-balanced papillary muscle • Tricuspid Regurgitation • Stretching of the originally noncircular tricuspid ring • Organic damage of tricuspid valve as a results of VSD patching • Failure of systolic leaflet coaptation 2001.7
Surgical Management for Failing Systemic RV • Double Switch Operation Correction of AV discordance and VA discordance simultaneously • Senning(Mustard) + ASO • Senning(Mustard) + Rastelli • Senning(Mustard) + REV • Conversion Switch Operation • previous atrial switch take-down and ASO 2001.7
Surgical Considerations • Left Ventricular Outflow Tract • Right Ventricular Size • Atrioventricular Valves • Ventricular Function • Heart Block and Arrhythmias • Coronary Arteries • Atrial Switch Operation • Reoperations • Potential Technical Problems for ASO • Timing of Operation • Role of Left Ventricular Retraining 2001.7
Proposed Patient Selection Criteria • Unobstructed LV to PA and RV to aortic connections • Balanced ventricular and AV valve sizes • Septatable heart, without major AV valve straddling • Translocatable coronary arteries • Current(or recent) LV/RV pressure ratio greater than 0.7 • Competent mitral valve with good LV function (Karl TR, et al. ATS 1997) 2001.7
Preparation for Systemic Left Ventricle • Naturally occurring preparation • Pulmonary Artery Banding • age • banding(LV retraining) duration • Preoperative Selection Criteria • Age • Wall thickness • LV/RV pressure ratio 2001.7
Senning Procedure 2001.7
Mustard Procedure 2001.7
Senning Plus Arterial Switch Operation for Congenitally Corrected Transposition (TR Karl, et al. Ann Thorac Surg 1997) • From 1989 to 1996 • 14 Senning + ASO : age ranged 0.5 to 120mo • 1 hospital Mortality • Actuarial survival beyond 10 months : 81% • Median grade of TR : preop ¾ to ¼ postop • Normal RV function : 11/12 current survivors 2001.7
Results of the Double Switch Operation in the Current Era (Imamura, et al. Ann Thorac Surg 2000) • From 1993 to 1998 • 22 Double Switch Operations in 27 CCTGA patients : age ranged 3mo to 55yrs • Senning & ASO : 10 • Senning & Rastelli : 12 • No early and late Mortality • Epicardial pacemaker insertion in 2 • Significantly improved degree of TR with normal LV and RV function 2001.7
Systemic Right Ventricular Failure After Atrial Switch Operation: Midterm Results of Conversion Into an Arterial Switch (Daebritz SH, et al. Ann Thorac Surg 2001) • 4 patients age 38 to 59 months of RV failure underwent arterial switch operation • previous operation : Senning and VSD closure • 1 late death(43.5 mo follow up) due to LV dysfunction • Survivors : improved FS, NYHA class I – II • Conversion switch operation is an alternative to cardiac transplantation in children • Long-term morbidity is caused by rhythm disturbance 2001.7
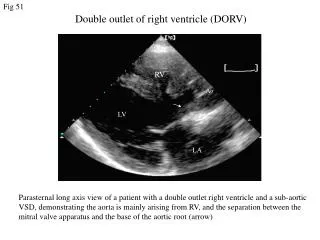
Experience in SNUCH • From 1990 to 2001 • 20 double switch operations • 1 conversion switch operation • Age : ranged 1month to 16 years (mean 46months) • M : F = 11 : 9 • Dx : CCTGA(with VSD, PS or PA) – 18 DORV, PS, VSD – 2 dTGA, VSD – 1 (Conversion switch after Senning procedure) 2001.7
Experience in SNUCH • Preop. procedures • PAB : 2 • LMBTS : 3 • RMBTS : 1 • LMBTS + RMBTS : 2 • VSD closure : 2 • BAS : 1 • PPM insertion : 1 • RV-PA conduit interposition : 1 2001.7
Experience in SNUCH • Operative technique • Senning + ASO : 6 • Senning + Rastelli : 9 • Mustard + ASO : 1 • Mustard + Rastelli : 1 • Senning + REV : 2 • Mustard + REV : 1 • * 1 conversion arterial switch operation after Senning and PAB 2001.7
Experience in SNUCH • Operative mortality : 7 (33%) • Number of death according to period • 1990 - 1993 : 5 (23.8%) / 10 initial learning period LCOS 4 / sepsis 1 * 3 immediate myocardial failure • 1994 - 2001 : 2 (9.5%) / 11 LCOS 1 / sepsis 1 2001.7
Experience in SNUCH • Complications • Postop. AV block : permanent pacemaker insertion in 3 • Chylothorax in 4 • Reoperation in 3 • Senning pathway reaugmentation • Redo Rastelli op d/t residual PS • Conduit change with Homograft 2001.7
Experience in SNUCH • Overall outcomes • Postoperative TR : all survivors in minimal or grade I • Preserved postoperative ventricular function in survivors : NYHA functional class I or II 2001.7
Operative Technique 2001.7
Conclusion • Double switch operation in selected patients in optimal anatomic & physiologic subsets has encouraging early outcomes with its theoretical advantage. • TR and subsequent RV dysfunction represent the major risk factor for CCTGA patients. • Conversion switch operation can be performed with acceptable risk and may provide long-term survival advantage if adequate patient preparation is warranted. 2001.7