Download
1 / 1
10 likes | 135 Views
Clinical Characteristics and Outcomes of Patients with Ischemic Cardiomyopathy and Persistent Angina Pectoris: From the Duke Databank for Cardiovascular Disease Robert J. Mentz , Samuel Broderick, Linda K. Shaw, Karen Chiswell, Mona Fiuzat, and Christopher M. O'Connor

E N D
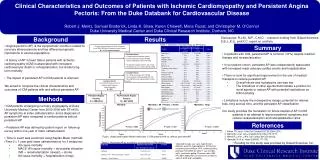
Clinical Characteristics and Outcomes of Patients with Ischemic Cardiomyopathy and Persistent Angina Pectoris: From the Duke Databank for Cardiovascular Disease Robert J. Mentz, Samuel Broderick, Linda K. Shaw, Karen Chiswell, Mona Fiuzat, and Christopher M. O'Connor Duke University Medical Center and Duke Clinical Research Institute, Durham, NC Results Disclosures: R.J.M., M.F., C.M.O. - research funding from Gilead Sciences. S.B.,L.K.S., and K.C. report no conflicts. Background Results Conclusions Table 1. Baseline Characteristics by AP Status. • Angina pectoris (AP) is the symptomatic condition related to coronary atherosclerosis and has different prognostic implications in various populations • A history of AP in heart failure patients with ischemic cardiomyopathy (ICM) is associated with increased cardiovascular death or rehospitalization, but similar long-term mortality • The impact of persistent AP in ICM patients is unknown Summary Cardiac Catheterizations at Duke University from 2000-2009 with Coronary Artery Disease N = 31,711 catheterizations Background • In patients with ICM, persistent AP is common (31%) despite medical therapy and revascularization • In our patient cohort, persistent AP was independently associated with increased major adverse cardiac events and hospitalization • There is room for significant improvement in the use of medical therapies to reduce persistent AP • Overall nitrate and hydralazine use was low • The limitations of other agents demonstrate a position for novel agents to reduce AP with potential implications on ICM morbidity • Limitations include the retrospective design, potential for referral bias, long accrual time, and the persistent AP classification • Our study provides the foundation for future studies of AP in ICM patients in an attempt to improve patients’ symptoms and reduce revascularization and rehospitalization rates • Excluded Patients: • Congenital Heart Disease (N=92) • Primary Valvular Disease (N=838) • AIDS or Metastatic Cancer (N=156) • No Baseline Angina Pectoris (N=7,741) • No follow-up to 1 yr after cath (N=1,825) • Excluded Patients: • EF ≥ 40% or unknown (N=19,796) • Non-ischemic cardiomyopathy (N=74) • Missing follow-up angina pectoris status (N=76) Analytical Cohort First Catheterization of 1,113 Patients with Ischemic Cardiomyopathy N = 965 We aimed to compare the clinical characteristics and outcomes of ICM patients with and without persistent AP Persistent Angina Pectoris N = 298 (31%) No Persistent Angina Pectoris N = 667 (69%) Methods Expressed as %, or median (Q1, Q3). * indicates P<0.05 Mortality + MI + Revasc + Stroke Mortality + Hosp Mortality • ICM patients undergoing coronary angiography at Duke University Medical Center from 2000-2009 with EF<40%, • AP symptoms at index catheterization, and a diagnosis of persistent AP were compared to similar patients without persistent AP • Persistent AP was defined by patient report on follow-up survey within one year of index catheterization • Time to event was examined using Kaplan-Meier methods (Time 0 = 1 year post index catheterization) for 3 endpoints: • All-cause mortality • MACE: All-cause mortality + myocardial infarction (MI) + revascularization (revasc) + stroke • All-cause mortality + hospitalization (hosp) Persistent AP No Persistent AP Event Probability References P-value = 0.588 P-value = 0.021 P-value < 0.0001 1. Fraker TD, et al. J Am CollCardiol 2007;50:2264-2274. 2. Mentz RJ, et al. Am J Cardiol 2012;109:1272-1277. 3. Mentz RJ, et al. J Am CollCardiol2013 [in press]. 3. Hjemdahl P, et al. Heart 2006;92:177-182. Years Years Years Figure. Unadjusted Kaplan-Meier event plots in ICM patients with vs. without persistent AP. * Funding for this study was provided by Gilead Sciences, Inc. Table 2. Persistent AP as a predictor of outcomes in ICM patients. *Adjusted for age, sex, race, hypertension, diabetes, prior MI, hyperlipidemia, NYHA class, cerebrovascular disease, PVD, smoking history, previous PCI/CABG (or within 1 year of index cath), ventricular gallop, Charlson Index, BMI, HR, SBP, medication use and serum creatinine, sodium, BUN and hemoglobin.






















