Download
1 / 47
480 likes | 520 Views
Discover the importance of the National Trauma Data Standard (NTDS) in enhancing patient care quality, benchmarking, and disaster preparedness. Learn about variability in data quality and the development of NTDS, with a focus on common variables and standardized coding conventions.

E N D
National Trauma Data Standard: Everything you’ve wanted to know but have been afraid to ask! N. Clay Mann, PhD, MS
Objectives • Need for a National Registry • The State of State Registries • Variability in Data Quality • Development of the NTDS • Implementation of NTDS
Need for a National Registry • Provide a national resource for clinical benchmarking, process improvement, and patient safety • Characterize all patient care • Provide baseline measures for enhancing disaster preparedness • Develop better injury scoring and outcome measures • This is not necessarily surveillance
States with Statewide Registries Planning – CA, DC, ID, KY, LA, ME, MA, MI, NE, NM, TN, WV, WI Technical Difficulties – ND, SD No Plans – HI, IN, NH, NJ, RI, VT
States with Registries • 27/32 require hospitals to report • 11 states…all acute care hospitals • 15 states…only designated centers • 1 state…only participating hospitals • 5/32 request hospitals report • 2 states…all acute care hospitals • 1 state…only designated centers • 2 states…partial registries
Threats to Data Integrity • Mandatory/elective Submission • Completeness of Case Capture • Difference in Case Definition • Difference in Coding Conventions
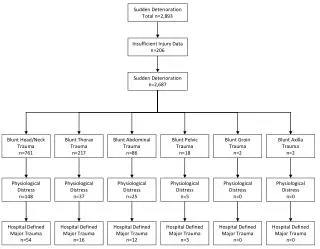
Variability in Case Definition Inclusion CriteriaNumberExclusion CriteriaNumber Abuse 4 Abuse 3 Blisters, contusions, Blisters, contusions, abrasions 3 abrasions 11 Drowning 13 Drowning 15 Smoke inhalation 7 Smoke inhalation 2 Foreign bodies 5 Foreign bodies 17 High altitude sickness 0 High altitude sickness 1 Lightning 5 Lightning 0 Same level fall 2 Same level fall 18 Poisoning 2 Poisoning 13
Variability in Case Definition • Variability in “same-level fall” exclusion • Same level fall AND age > 55 yrs old • Same level fall AND age > 65 yrs old • Same level fall AND isolated hip fracture (ICD-9 820) • Same level fall AND fracture of the vertebral column (ICD-9 805) • Same Level fall AND isolated fracture of the pelvis (ICD-9 808.2) • Same level fall AND superficial injury (ICD-9 910-924) • Same level fall AND age > 65 yrs old AND isolated hip fracture (ICD-9 820) • Same level fall AND age > 65 yrs old AND isolated extremity fracture (no ICD-9 codes listed)
Variability in Coding Conventions Glasgow Coma Score in ED • 15 states………..……initial GCS • 8 states……..initial and last GCS • 1 state………………...worst GCS • 1 state………………… best GCS • 1 state……..initial and worst GCS
Variability in Coding Conventions Time of Injury Coding ConventionNumber of States Report “Not documented” 10 Report EMS dispatch time 8 Report 5 minutes prior to EMS dispatch time 2 Report 15 minutes prior to EMS dispatch time 1 Report 5 to 20 minutes prior to EMS dispatch time depending on call location and general scene info 1 Report EMS dispatch time only if MVC§ 1 Report EMS arrival time 1 Report in categories (< 1 hour, 1-6 hours, 7-12 hours, 13-24 hours, or >24 hours) 1
Data Needs for Registries • All States with Trauma Registries • Complete Data Capture • Common Subset of Variables • Uniform Data Definitions and Values • Standardized Coding Conventions • Common Definition of Injury • Uniform Inclusion Criteria
Existing National Registry • Annual Report • NTDB Pediatric Report • NTDB Slide Kits • Hospital Benchmark Reports • Trauma Center Data Report Cards • ACS Bulletin Articles
2007 • NTDB contains over 2.7 million records • From 900 US trauma centers • Annual Report Version 7.0 released
Standard Inclusion Criteria Standard Data Definitions Standard Source Hierarchy Standard Comorbidities Pediatric specific additions Auto-Calculated Fields Edit Checks The “ Validator” National Trauma Data Standard
Ensuring Common Variables • Common Subset of Variables • Evaluate variable frequency across registries • Consider importance at national level • Seek consensus from experts
Variable Schema Primary Variable Supportive Variable Autogenerated Variable Secondary Variable
Auto-generated Variables • FIPS - like code (location code) • Trauma Type (blunt, penetrating, burn) • Injury Intentionality (using CDC matrix) • Total EMS Response Time • Total EMS Scene Time • Total EMS Time • Revised Trauma Score in the Prehospital Setting (adult and pediatric) • Revised Trauma Score in ED (adult and pediatric) • Abbreviated Injury Scale (six body regions) • Injury Severity Score • International Classification Injury Severity Score • Functional Capacity Index • Total ED Time • Total Length of Hospital Stay
Choosing Inclusion Criteria Uniform Inclusion Criteria • Collect all state inclusion/exclusion criteria • Assess criteria for commonalities • Look for least common denominator? States Criterion
National Trauma Data Standard THE “VALIDATOR” “Hasta La Vista Bad Data”
“Validator” External Server NTDS Outcomes “Validator” Benefit of a Common XML NTDB NEMSIS
Facility Demographics • Expanded Facility information screens • Hospital type • Hospital teaching status • Verification level • Bed Inventory • Inclusion criteria • Transfers in or out • Age of pediatric patients • Comorbidities and complications • Number of registrars • Number of surgeons • Software product utilized
Verification Requirement Annual NTDB participation Officially in effect with new green book Centers received waivers in 2007 as needed Year round data submission started in 2008
Call for Data 2008 First NTDB call for data based on NTDS version 1.2 Map current registry fields to the new standard 2009 Second NTDB call for data based on NTDS version 1.2 Updated software from vendors that incorporates all the new data fields and allows for direct data entry.
We need your support! • National Trauma Data Standard will: • Allow for seamless participation in NTDB • Describe severe trauma nationally • Characterize treatment and outcome • Assess trauma systems attributes • Link to standardized EMS data • Vendors are also interested in your commitment!
Technical Assistance • Visit the website • Join the NTDS Google Group • Talk with your software vendors • Utilize resources at the ACS and NEMSIS TAC
For More Information… • www.ntdb.org • www.ntdsdictionary.org • www.ntdbdatacenter.com
Additional Questions • Contact • N. Clay Mann clay.mann@hsc.utah.edu (801) 585-9161 • Melanie Neal MNeal@facs.org (312) 202-5536