Download
1 / 41
410 likes | 447 Views
Explore the evidence, clinical audits, intervention aims, treatment principles, and outcomes of managing chronic strongyloidiasis in Aboriginal communities. Learn how serology monitoring and effective treatment reduce risks, with ivermectin showing superior efficacy over albendazole.

E N D
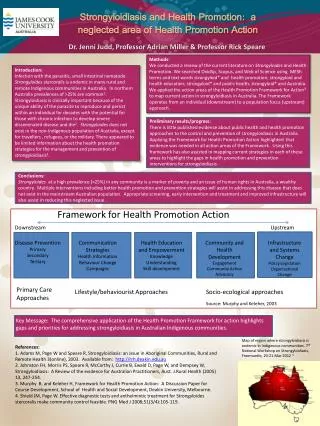
Miwatj Health Aboriginal Corporation Implementing best practice in the management of Strongyloidiasis Wendy PageKaren DempseyJames McCarthy
Background • 1995- JCU parasitology course in Nhulunbuy • 1996 - recognised as underlying diagnosis in clinical presentation (septicaemia, haemoptysis, meningitis, nephrotic syndrome, norwegian scabies etc) • 1999 – death of senior AHW from disseminated strongyloidiasis • 2001 – First National Workshop on Strongyloidiasis in Nhulunbuy
What is the evidence for high prevalence in Aboriginal communities? • Community based faecal surveys (Low sensitivity) • NT -East Arnhem 1993 – 41% • NT- Elcho Island 1995 – 15% • Qld -Woorabinda 1995 – 15% • Qld- Doomadgee 1992 – 14% (<15yrs old) • WA - Gibb River Rd communities 2000 – 25% • NSW -Central coast – 4.9% • NSW- Northern Rivers 1960’s – 30%
NT - Children admitted with diarrhoea to Royal Darwin Hospital 2000 (<5yo) • 7.2% • all cases from remote areas • wasting, hypokalaemia and prolonged hospital stay • Comparison with serology – false negatives reflecting a window period and no false positives
Top End Division of General Practice Strongyloidiasis Clinical Audit 2001 • Patients with eosinophilia • Urban- 6% • Remote – 37% • Patients with eosinophilia and tested for strongyloidiasis • 56% pos ELISA • 16% equivocal • 28% negative
Aim of Intervention • Implementation of best practice management of Chronic Strongyloidiasis in an endemic Indigenous community • Identify patients with chronic strongyloidiasis before they present with serious clinical manifestations
Principles of Best Practice Management of Strongyloidiasis • Treat all infected cases even if no symptoms as fatal hyperinfection is unpredictable • Every attempt must be made to eradicate the parasite because of its ability to replicate (autoinfective cycle) • Refer to Harrison’s Principles of Internal Medicine and Oxford Handbook of Tropical Medicine
Strongyloidiasis Care Plan • Diagnose: • Strongyloides IgG EIA (ELISA) serology is a sensitive diagnostic test for chronic strongyloidiasis • Incorporate into adult primary health care program (Biennial health check) • Treatment • 1995 -Albendazole 400mg for 3days Repeat at 7 days • 2000 - Ivermectin 200mcg/kg (12mg) • Follow upStrongyloides specific IgG EIA serology at 6 months and 12 month
Is Strongyloides specific IgG EIA serology a useful tool for monitoring the effectiveness of treatment in an endemic Indigenous community?
Methodology • An observational study involving an audit of the Miwatj Health Aboriginal Corporation health data base (Ferret) • Seropositive cases • Treatment • Follow up serology after treatment
Initial Seroprevalence • 508 tested using Strongyloides IgG EIA serology during the period 1996-2002 • 250 negative (49%) • 81 equivocal (16%) • 177 positive (35%)
Results: Albendazole vs Ivermectin • Only 10 declined to negative with Albendazole (1996-2003) • 69 treated with Ivermectin and followed up(2000-2003) • 62 (90%)declined to negative • 5 (7%)declined to equivocal • 2 (3%)remained positive
Comparison of treatments A1 vs A3 p=0.02 A1 vs Ivermectin p<.00001 A3vs Ivermectin p=0.02
Conclusions • Strongyloides IgG EIA serology is a useful tool to monitor effectiveness of treatment in endemic communities • A positive Strongyloides IgG serology result does not indicate past infection • “Past” infection occurs when the patient is asymptomatic, negative stool and low negative serology. • Ivermectin is more effective than albendazole
Conclusions • Including Strongyloides serology in biennial adult health surveillance in endemic areas is • a cost effective intervention • identifies adults with chronic strongyloidiasis, • provide effective treatment and • reduce risk of serious clinical manifestations • Reduces the human reservoir of infection
Conclusions • Best Practice management for chronic strongyloidiasis in individuals in non-endemic communities is also applicable for individuals in endemic Indigenous communities in Australia • Treating the infected population will decrease transmission (no human reservoir == no transmission)
Transactions of the Royal Society of Tropical Medicine and Hygiene (2006) 100, 1056-1062. • Utility of serologic follow-up of chronic strongyloidiasis after anthelminthic chemotherapy • Page WA, Dempsey K, McCarthy JS
Results: analysis of changes in Strongyloides- specific IgG in 79 seropositive cases in endemic Indigenous community • Multiple courses of ivermectin 35/42 – 83% • Single course ivermectin 13/19 – 68% • Multiple courses of albendazole 7/10 – 70% • Single course 3 days of albendazole4/10- 40% • Single dose of albendazole 0/5 – 0% • No documented treatment 1/10 – 10% • Directly observed therapy
Thank you • Inspired by courage of Indigenous persons • Miwatj Health Aboriginal Corporation – board, management, heath staff and including Marngarr and Laynhapuy • RACGP, ACRRM, ARDS,JCU. • Centre for Remote Health and MICRRH • Team support from experts on Strongyloides • ASM- Robyn Wood, Andrew Butcher • National Strongyloides Working Group
Diagnosis • Strongyloides IgG EIA (ELISA) serology is a sensitive diagnostic test for chronic strongyloidiasis • Low cost and useful to monitor cure • Faeces insensitive and labour intensive • Agar plate most sensitive faecal culture technique
CHRONIC STRONGYLOIDIASIS TREATMENT & FOLLOW-UP FLOW CHART Baseline Strongyloides Serology Positive Negative Equivocal NO TREATMENT Test for pregnancy Rx with Ivermectin (if from endemic area) Rx with Ivermectin x2 Follow-up serology and eosinophil count at 6 months after treatment Negative Still Positive Decreasing serology and negative eosinophilia NO TREATMENT Retreat with 3 doses of Ivermectin one month apart Follow up serology at 6 months Negative Still Positive NO TREATMENT Medical Review Review 2 yearly to confirm eradication or if at higher risk for reinfection Based on recommendations from Second National Workshop on Strongyloidiasis, July 2003
“ We’ve had this strongyloides for so long, why hasn’t something been done about it?” Senior Indigenous Participant at First National Workshop on Strongyloidiasis September, 2001.
Miwatj Indigenous Women’s Conference September 2001 • Strongyloidiasis • Recommendation 29 – Miwatj Indigenous Women’s Conference recommends that there be more education provided on the issues of Strongyloidiasis and hygiene to each community. • Recommendation 30 – Miwatj Indigenous Women’s Conference recommends that screening for Strongyloidiasis be conducted in all communities.
“One of the aims of Miwatj Health Aboriginal Corporation is to improve health outcomes so that we can more closely approach the life expectancy of mainstream Australians. • An obvious step along the way is to eradicate a disease that is common in remote Indigenous communities, a disease rarely experienced by mainstream Australians.” • Andrea Collins, Second National Workshop on Strongyloidiasis July 2003.
CARPA Manual – need to update • Who to test for strongyloides serology • High risk groups • Household contacts of positive cases (Conway) • People who will be started on immunosuppressants • People who will be started on corticosteroids (one dose has been documented to precipitate disseminated strongyloidiasis – dysregulation) • People with symptoms who have lived in wet tropics • People with unexplained high eosinophil count • People who have been treated and are being followed up (6 months after treatment) to assess if further treatment is needed
CARPA manual – need to updateStrongyloides treatment • Treat if positive by stool test • Treat if positive or equivocal serology • Person from high risk group who is to receive specialist treatment that will weaken their immune system even if their serology is negative • Children less than 5yo Albendazole 3/7 rpt 1week • Children more than 5yo and adults: Ivermectin repeat after 1 week. • Follow up patients with serology and retreat if required.
CARPA Manual – need to update • Cyclosporin acts as antiparasitic • Septicaemia not rare in endemic areas
Who dies from strongyloidiasis? • Patients in high risk groups and no tests done for Strongyloides • Patients with clinical signs (esp, recurrent unexplained sepsis, haemoptysis, rashes) and no tests done • Patients with “cured” strongyloidiasis and no follow-up • Patients diagnosed with strongyloidiasis and significance missed • Immunosuppressed patients with no tests done
100 million worldwideHigh Risk Groups in Australia(exposure may be decades earlier) • Indigenous Australians (esp Northern Australia to central coast NSW) • Military War Veterans • WW2 esp ex POW (37% pos in 1980s) • Vietnam War vets (1 – 5%) • Immigrants and refugees • Returned travellers – “A souvenir you don’t want to bring home” • Sanitation workers
Key Distinguishing features of Strongyloides stercoralis • Autoinfective cycle allows chronic infection to remain for decades without reinfection from outside. This results in chronic strongyloidiasis. • Once infected always infected (even after treatment) unless proven otherwise.- Lim & Biggs, MJA 2001 • Autoinfective larvae carry bacteria from the bowel and may invade any organ of the body including the CNS • Hyperinfectionis unpredictable and high fatality rate(80%) • Prescribing of steroids or immunosuppressants may precipitate fatal disseminated strongyloidiasis – the autoinfective cycle is stimulated (Corticosteroids implicated with over 60% of fatal cases of disseminated strongyloidiasis)
CARPA reference manual • PPV&NPV dependent on prevalence- higher the prevalence, the higher the PPV • Community control strategies • “ infection is likely to disappear from a community with improving socioeconomic status as the environmental reservoir diminishes and infected population ages and dies” is not a quote from Conway!