Download
1 / 3
30 likes | 134 Views
This overview explores the metabolic pathway of steroids, emphasizing their water solubility post-liver conjugation and subsequent renal excretion. It discusses the diverse actions of a single hormone on target cells through modifications in the cytoplasm and nucleus. Key topics include steroidogenesis starting from cholesterol, the potency variations among estrogen types, and the clinical implications of hormone therapies. The role of selective estrogen receptor modulators and the risks associated with hormone treatments such as DVT and endometrial cancer are also examined.

E N D
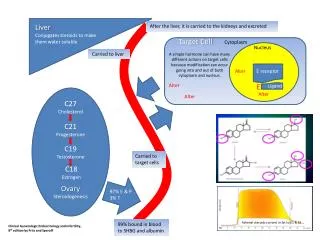
Liver Conjugates steroids to make them water soluble After the liver, it is carried to the kidneys and excreted Target Cell Cytoplasm Nucleus Carried to liver A simple hormone can have many different actions on target cells because modification can occur going into and out of both cytoplasm and nucleus. Alter E receptor Alter E Ligand Alter Alter C27 Cholesterol C21 Progesterone C19Testosterone Carried to target cells C18Estrogen Ovary Steroidogenesis 97% E & P 3% T Adrenal steroids convert in fat to E1 & E2 99% bound in blood to SHBG and albumin Clinical Gynecologic Endocrinology and Infertility, 8th edition by Fritz and Speroff
Female HormonesTrue or False • Steroidogenesis starts with cholesterol. • Steroidogenesis cleaves carbon atoms from cholesterol to make progesterone, testosterone, and estrogen. • Blood binding of steroids acts to buffer and extend the life of naturally occurring steroids. • Target cells modify steroids as they enter and as they leave both the cytoplasm and the nucleus of cells. • The liver conjugates and makes steroids water soluble. • The kidney excretes steroids once they are water soluble. • 30% of female estrogen is from adrenal steroids converting in fat to estradiol and estrone. • Estradiol is 12 times as potent as Estrone and 80 times as potent as Estriol. • The ethinyl group, a triple bonded carbon pair, allows oral administration of estrogen when attached to estrogen as ethinyl-estradiol by stabilizing it through the harsh stomach environment. • Selective Estrogen Receptor Modulators, SERMs, as not estrogen. • Unopposed estrogen increases the risk of endometrial cancer from 1/1000 to 1/400, RR 2.4. • Postmenopausal estrogen does not increase the risk of breast cancer according to the Women’s Health Initiative. • Postmenopausal progesterone does increase the risk of breast cancer according to the Women’s Health Initiative. • ER and PR positive breast cancers do better, in general, than ER and PR negative breast cancers. • Tamoxifen, a SERM, down-regulates breast estrogen effect but acts as a pure estrogen on the endometrium.
Female HormonesTrue or False • To stop heavy uterine bleeding, consider Premarin 10 mgm IV q 2 hours in the hospital. It works buy increases DVT risk and may cause hemorrhage later. • To stop heavy uterine bleeding, progesterone is preferred if you have a few days to slow the bleeding. • #2 results in more uterine spotting, but does not increase the risk of DVT and is usually a permanent fix to the problem. • #2 - A birth control pill cycle pack of 21 pills can be taken 1 PO QID, then TID, then BID, then QD until finished. Birth control pills contain mostly progesterone but, also, some estrogen. • #2 – Progesterone 10 mgm daily can be used the last 10 days of each cycle. “Take one a day for 10 days starting a week before you think your period will start.” • Premarin is extracted from horse’s urine and does NOT contain estradiol. • Testosterone is not used to decrease endometrial bleeding because it does not down-regulate estrogen receptors.