Download
1 / 52
520 likes | 644 Views
MRC Centre for Neuromuscular Disease. Neuropathy and Waldenström's Macroglobulinaemia London January 2011. Dr Michael Lunn Consultant Neurologist and Clinical Lead in Neuroimmunology National Hospital for Neurology and Neurosurgery Queen Square London WC1N 3BG

E N D
MRC Centre for Neuromuscular Disease Neuropathy and Waldenström's MacroglobulinaemiaLondon January 2011 Dr Michael Lunn Consultant Neurologist and Clinical Lead in Neuroimmunology National Hospital for Neurology and Neurosurgery Queen Square London WC1N 3BG michael.lunn@uclh.nhs.uk
Neuropathy and Waldenström's Macroglobulinaemia • What is a nerve? • What is a neuropathy? • What are the symptoms and signs? • How is it diagnosed? • Why and how does Waldenstrom’s cause neuropathy? • What can be done about it? Treatment. • Where might I find out more?
A nerve conducts electrical impulses around the nervous system
A nerve conducts electrical impulses around the nervous system
Nerve from real life – normal and damaged Normal nerve CIDP Brandner S - NHNN
The nerve cell surface is covered in ‘targets’ for antibodies
Neuropathy and Waldenstrom’sMacroglobulinaemia • What is a nerve? • What is a neuropathy? • What are the symptoms and signs? • How is it diagnosed? • Why and how does Waldenstrom’s cause neuropathy? • Are there any similar conditions? • What can be done about it? • Where might I find out more?
What is a neuropathy? • A neuropathy is present when a peripheral nerve is damaged • There are many causes of peripheral neuropathy • Compression (carpal tunnel syndrome) • Diabetes • Toxins (e.g. alcohol) and vitamin deficiencies • Infections (e.g. leprosy) • Inflammatory causes
Neuropathy represents damage to the myelin sheath or the axon
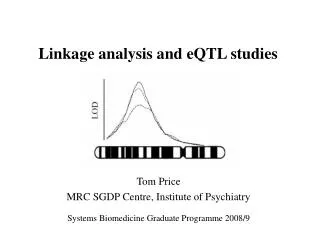
How common is it?Prevalence (per 100,000)Martyn CN and Hughes RAC Peripheral Neuropathies in Epidemiology of Neurological Disorders BMJ 1997 All types 2400 Carpal tunnel 5800 f 600 m Diabetic 300 HMSN 8 - 41 CIDP and Waldenström's > 1
Neuropathy and Waldenstrom’sMacroglobulinaemia • What is a nerve? • What is a neuropathy? • What are the symptoms and signs? • How is it diagnosed? • Why and how does Waldenstrom’s cause neuropathy? • Are there any similar conditions? • What can be done about it? • Where might I find out more?
Positive Pins and needles Pain Muscle twitching Cramps Restlessness Tremor Negative Loss of sensation – numbness Weakness Wasting Symptoms of peripheral neuropathy
Signs of peripheral nerve disease • Weakness • Wasting • Loss of reflexes • Sensory loss • Ataxia (unsteadiness) • Thickening of nerves • Skin changes • Consequences of sensory loss – ulcers, arthropathy • Others
Distal wasting Courtesy of imagesMD Taken from: Thomas D. Bird, S. Mark Sumi In Atlas of Clinical Neurology: Clinical Neurology. Edited by Roger N. Rosenberg. Current Medicine, Inc. 2000
Neuropathy and Waldenstrom’sMacroglobulinaemia • What is a nerve? • What is a neuropathy? • What are the symptoms and signs? • How is a neuropathy diagnosed? • Why and how does Waldenstrom’s cause neuropathy? • Are there any similar conditions? • What can be done about it? • Where might I find out more?
How do we diagnose a neuropathy? • Clinical symptoms and patient characteristics • Clinical signs on examination • Neurophysiological testing • nerve conduction studies and electromyography • Special blood tests
B A Conduction velocity = A/B ms-1
Anti-MAG paraproteinaemic demyelinating peripheral neuropathy (PDPN) • Chronic progressive sensorimotor demyelinating neuropathy • Older person (average 65-75 years), male • Numb in feet and unsteady • Tremor of hands (sometimes mild, sometimes worse) • Ataxic (unsteady) walking • IgM paraprotein in serum • Paraprotein has ‘anti-MAG’ activity • The antibody ‘sees’ a nerve sugar on MAG called HNK-1 • also on some other nerve molecules but MAG most likely • Characteristic pathology
Neuropathy and Waldenstrom’sMacroglobulinaemia • What is a nerve? • What is a neuropathy? • What are the symptoms and signs? • How is it diagnosed? • Why and how does Waldenström's cause neuropathy? • Are there any similar conditions? • What can be done about it? • Where might I find out more?
Inflammatory Peripheral Neuropathy Idiopathic Va sculitic Neuropathy Acute Acute inflammatory demyelinating polyradiculoneuropathy (AIDP) Acute motor axonal neuropathy (AMAN) Primary vasculitis Acute motor - sensory axonal neurop athy (AMSAN) Polyarteritis nodosa and Churg - Strauss disease Fisher Syndrome and other regional variants Wegener’s vasculitis Pharyngeal - cervical - brachial Isolated nerve vasculitis Paraparetic Temporal arteritis Facial palsies Systemic autoimmune diseases with associated vasculitis Pure oculomotor Rheumatoid arthritis Functional variants of GBS Systemic lupus erythematosus Pure dysautonomia Sjörgren’s syndrome Pure sensory GBS Mixed connective tissue disease Ataxic GBS Other Subacute Serum sickness Subacute inflammatory demyelinati ng polyradiculoneuropathy (SIDP) Infectious, malignant, related to chemotherapy Chronic Inflammatory neuropathy associated with infection Chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) Multifocal motor neuropathy with conduction block (MMNCB) HIV neuropathies, including CMV neuropathy Chronic relapsing axonal neuropathy Leprosy Chronic ataxic sensory neuronopathy Lyme disease Chaga’s disease Paraproteinaem ic neuropathy Paraneoplastic Monoclonal gammopathy of undetermined significance (MGUS) Multiple myeloma Sub - acute sensory neuropathy/neuronopathy - small cell lung Solitary plasmacytoma carcinoma and anti - Hu Abs Lymphoma or chronic lymphocytic leukaemia Other paraneoplastic tumour - antibody syndromes Waldenström’s macroglobulinaemia Cryoglobulinaemia Metabolic Cold agglutinin disease Primary amyloidosis Diabetic lumbo - sacral plexopathy POEMS syndrome
Waldenström's causes an ‘inflammatory’ neuropathy Paraprotein associated neuropathies part of group of inflammatory neuropathies Inflammatory neuropathies have presumed ‘immune mediated’ pathogenesis Inflammatory cells infiltrate nerves and damage myelin and/or axons
The IgM in Waldenström's sometimes targets Myelin Associated Glycoprotein (MAG) MAG
Myelin Associated Glycoprotein (MAG) A myelin sugar-protein 1% brain protein 0.1% nerve proteins MAG is localised in specific sites on the myelin surface MAG associates with other signalling molecules that control the axon and the myelin MAG normal functions Cell-cell recognition signal transduction through the membrane, myelin-axon inter-communication
Conclusions • Neurofilaments are significantly closer in diseased axons from patients with anti-MAG paraproteins. • We think that thinned nerves are not able to transport substances so easily • This leads to damage to the ends of the nerves • Treating earlier may be of benfit but we don’t know for definite
IgM paraproteinaemic (anti-MAG) neuropathy treatment Is treatment required at all? Do you need to treat the Waldenström's? IVIG confers short term benefit – RCT Multiple other immunosuppressants used Melphalan, chlorambucil, cyclo +/- steroid, fludarabine
Rituximab (anti-CD20) – promising in some studies • 8 studies – 6 (79 pts) positive (1 (3 pts) negative) • 3 fully published, 2 not adequately controlled • 1 Randomised trial published (Dalakas 2009) with serious flaws – reported ‘positive’ • Another trial completed – mixed results • 375mg/m2 usual dose – recent high dose study added improvement • Some published cases of worsening • We give in close discussion with haematology services
Mechanisms of B-cell Functions Dalakas M Neurology 2008;70:2252
B cell development 2 Dalakas M 2008 Nature
Rituximab Chimeric (Mouse-human) anti-CD20 antibody 1st monoclonal approved for use in cancer (1997) Depletes CD20 +ve cells in hours to days for 8-12months
Rituximab - Safety • 84% infusion reactions – 97% mild • 30% post infusion infection – 1-2% severe • Maintained Ig levels and T-cell function • Concomitant anti-T-cell therapy hazardous • Serious infections more common with concomitant illness/immunosuppression • PML • 2 cases in SLE treated with Rituximab (+ additional immunsuppressants) • 23 cases in neoplasia Rx with Rituximab • HACA antibodies uncommon • Some high titre, more common in AI disease • Effects unclear – may cause depletion failure
Other treatments • Not usually painful – pain medications • Physiotherapy for walking and balance • Foot care • Walking and balance aids • Ankle foot orthoses • Sticks • Walkers • Driving advice
Where might I find out more? • GBS Support Group • http://www.gbs.org.uk • GBS-CIDP Foundation International • http://www.gbs-cidp.org/ • The Neuropathy Trust • http://www.neurocentre.com/