Download
1 / 69
690 likes | 783 Views
Acquired valve diseases. Prof. S. Smiyan. EPIDEMOLOGY. ARF is mainly a disease of children aged 5–14 years. Initial episodes become less common in older adolescents and young adults and are rare in persons aged >30 years.

E N D
Acquired valve diseases Prof. S. Smiyan
EPIDEMOLOGY • ARF is mainly a disease of children aged 5–14 years. • Initial episodes become less common in older adolescents and young adults and are rare in persons aged >30 years. • There is no clear gender association for ARF, but RHD more commonly affects females, sometimes up to twice as frequently as males.
Caused by group A streptococcus. There is a latent period of ~3 weeks (1–5 weeks) between the precipitating group A streptococcal infection and the appearance of the clinical features of ARF. ORGANISM
PATHOGENESIS • Rheumatic fever affect the peri-arteriolar connective tissue and can occur after an untreated Group A streptococcal pharyngeal infection. • It is believed to be caused by antibody cross-reactivity. This cross-reactivity is a Type II hypersensitivityreaction and is termed molecular mimicry
Characteristic Aschoff bodies, composed of swollen eosinophilic collagen surrounded by lymphocytes and macrophages can be seen on light microscopy.
In acute RF, these lesions can be found in any layer of the heart and is hence called pancarditis. The inflammation may cause a serofibrinous pericardial exudates described as “bread-andbutter” pericarditis, which usually resolves without sequelae
Nimishikavi S, Stead L Streptococcal Pharyngitis – Images in Clinical Medicine. NEJM 2005: 352:e10.
Arthritis: This is usually polyarthritis, sometimes flitting from joint to joint (migratory), affecting the larger joints more than the smaller ones. Swelling, redness and tenderness are the common findings and occasionally joint effusions.
Skin lesions : The classical erythema marginatum—large erythematous lesions with prominent margins slightly raised. The red margins take longer to fade and so the lesions sometimes look like red rings
Subcutaneous nodules : These are painless, roundish, firm lumps overlaid by normal looking skin They range from a few millimeters to 1.5 cm in diameter, and are localised over bony prominences like the elbow, shin and spine. They sometimes last longer than a month.
Up to 60% of patients with ARF progress to RHD. The endocardium, pericardium, or myocardium may be affected. Valvular damage is the hallmark of rheumatic carditis. The mitral valve is almost always affected.
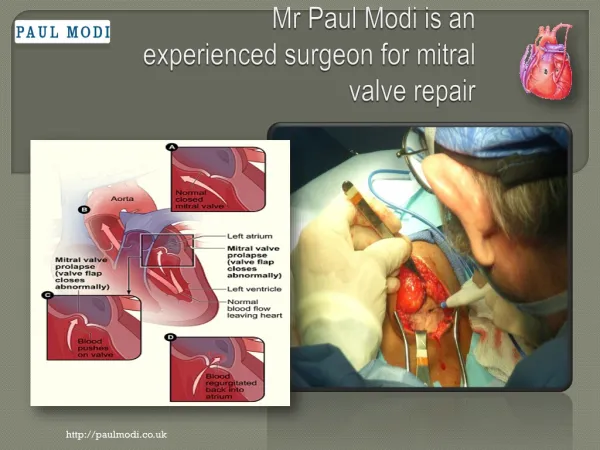
Rheumatic heart disease. Abnormal mitral valve. Thick, fused chordae
Another view of thick and fused mitral valves in Rheumatic heart disease
It presents with breathlessness, chest pain of pericardial type, and palpitations due to tachycardia. a soft mid-diastolic murmur due to thickening of the mitral valve, the Carey-Coombs murmur, is the classical picture; Pericardial rub may be heard at some stage in the disease.
Sydenham's chorea commonly occurs in the absence of other manifestations, follows a prolonged latent period after group A streptococcal infection, The choreiform movements affect particularly the head (causing characteristic darting movements of the tongue) and the upper limbs They may be generalized or restricted to one side of the body (hemi-chorea). Chorea eventually resolves completely, usually within 6 weeks.
Jones Criteria (1993) • Major manifestations: Arthritis (70%) – involves large joints simultaneously or in succession; responds dramatically to salicylates Carditis (50%) – includes some or all of the following in increasing order of severity:Tachycardia (out of proportion to the fever) – its absence makes the diagnosis of myocarditis unlikely Heart murmur of valvulitis – MR or AR Pericarditis – friction rub, pericardial effusion, chest pain, ECG changes Cardiomegaly – seen on chest X-ray Signs of CHF – gallop rhythm, distant heart sounds, cardiomegaly Valvulitis – murmurs Myocarditis – unexplained cardiomegaly or CHF or gallop Pericarditis – friction rub or pericardial effusion Miscellaneous findings – conduction disturbances in the ECG; 2D echo findings Erythema marginatum (<10%) – nonpruritic serpiginous or annular erythematous evanescent rashes most prominent on the trunk and inner proximal portions of the extremities; never on the face (disappear on exposure to cold and reappear after a hot shower or if covered with a blanket); blanches on pressure Subcutaneous nodules (2-10%) – particularly seen in recurrent cases; hard, painless, nonpruritic, freely movable swellings 0.2-2 cm in diameter; found symmetrically, singly or in clusters on the extensor surfaces of large & small joints, over the scalp or along the spine; last for weeks Sydenham’s chorea (15%) – occurs more often in prepubertal girls; consist of choreic movements (spontaneous purposeless movements followed by motor weakness),hypotonia, emotional lability, hyperactivity, separation anxiety, obsessions & compulsions; may be related to dysfunction of BG & cortical neurons; increased titers of “antineuronal antibodies” in >90%
Jones Criteria (1993) • Minor manifestations: • Arthralgia – not considered a minor manifestation if arthritis is present • Fever – at least 38.8 C • Elevated acute phase reactants (CRP and ESR) • Prolonged PR interval on the ECG
EVIDENCE OF ANTECEDENT GROUP A STREPTOCOCCAL INFECTION • History of sore throat/scarlet fever unsubstantiated by lab. data is not adequate evidence of recent infection. • A negative rapid strep antigen detection test should be confirmed by a conventional throat culture. • Streptococcal antibody tests are the most reliable lab.evidence. The onset of the clinical manifestations coincide with the peak of the streptococcal antibody response.
Treatment • Step I- primary prevention (eradication of streptococci) • Step II- anti inflammatory treatment (aspirin,steroids) • Step III- supportive management & management of complications • Step IV- secondary prevention (prevention of recurrent attacks)
STEP I: Primary Prevention of Rheumatic Fever (Treatment of Streptococcal Tonsillopharyngitis) Agent Dose Mode Duration Benzathine penicillin G 600 000 U for patients Intramuscular Once 27 kg (60 lb) 1 200 000 U for patients >27 kg or Penicillin V Children: 250 mg 2-3 times daily Oral 10 d (phenoxymethyl penicillin) Adolescents and adults: 500 mg 2-3 times daily For individuals allergic to penicillin Erythromycin: 20-40 mg/kg/d 2-4 times daily Oral 10 d Estolate (maximum 1 g/d) or Ethylsuccinate 40 mg/kg/d 2-4 times daily Oral 10 d (maximum 1 g/d) Recommendations of American Heart Association
Step II:Anti inflammatory treatment Clinical condition Drugs
Bed rest Treatment of congestive cardiac failure: -digitalis,diuretics Treatment of chorea: -diazepam or haloperidol Rest to joints & supportive splinting 3.Step III: Supportive management & management of complications
STEP IV : Secondary Prevention of Rheumatic Fever (Prevention of Recurrent Attacks) Agent Dose Mode Benzathine penicillin G 1 200 000 U every 4 weeks* Intramuscular or Penicillin V 250 mg twice daily Oral or Sulfadiazine 0.5 g once daily for patients 27 kg (60 lb Oral 1.0 g once daily for patients >27 kg (60 lb) For individuals allergic to penicillin and sulfadiazine Erythromycin 250 mg twice daily Oral *In high-risk situations, administration every 3 weeks is justified and recommended Recommendations of American Heart Association
Duration of Secondary Rheumatic Fever Prophylaxis Category Duration Rheumatic fever with carditis and At least 10 y since last residual heart disease episode and at least until (persistent valvar disease*) age 40 y, sometimes lifelong prophylaxis Rheumatic fever with carditis 10 y or well into adulthood, but no residual heart disease whichever is longer (no valvar disease*) Rheumatic fever without carditis 5 y or until age 21 y, whichever is longer *Clinical or echocardiographic evidence. Recommendations of American Heart Association
Mitral Stenosis • Etiology: predominant cause: rheumatic fever rare cause • Pathology: thickening, shortening, adhering, calcium depositing, and scarring four forms of fusion: (1) commissural, (2) cuspal, (3)chordal, (4)combined two types of shape: fish-mouth shaped, funnel-shaped
Mitral Stenosis • Pathophysiology: normal cross-sectional area: 4-6 cm2 mild MS: <2 cm2, LAP↑→LAH ---compensated period moderate MS: <1.5 cm2, PVP↑, PCWP↑, →interstitial edema severe MS: <1.0 cm2,PAP↑→RVoverload →RV failure →TR →PR
Mitral Stenosis • Clinical Manifestations (MVA<1.5cm2) 1. Symptom: dyspnea, hemoptysis, cough, hoarseness (ortner’s syndrome) 2. Signs: -Mitral faces -Diastolic thrill at apex -S1↑(flexible), OS(Opening snap), Diastolic rumbling murmur at apex, -P2↑, splitting, Graham-Steel murmur(PR),TR
Mitral Stenosis • Laboratory Examination - ECG: 1) left atrial enlargement: P wave (II,V1) 2) Af; 3) right ventricular hypertrophy - X-film: change in cardiac silhouette, Kerley B lines - Echocardiography: M-mode, Two- dimensional, Doppler
Physical examthe murmur • "Tapping" sensation over area of expected PMI. • Accentuated S1 • Opening snap. • Mid-diastolic murmur (rumble) low in pitch. • S2-OS interval of 70 msec is seen in severe MS. • Best heard after exercise, left lateral recumbency. • Bell chest piece lightly applied. • Pulmonary HTN and RVF occur later in MS. Low sensitivity • P mitrale: • Lead II broad and bifid > 0.12 sec • Lead V1 broad and deep negative component of biphasic P wave, longer than 0.04 sec and 1 mm in depth. • If pulmonary hypertension is present, tall peaked P waves, right axis deviation, or right ventricular hypertrophy appears. • Atrial fib. • Atrial flutter.
CXR • Straight left heart border. • Large left atrium. • Sharply indenting esophagus. • Elevation of left mainstem bronchus. • Large right ventricle and pulmonary artery if pulmonary hypertension is present. • Calcification occasionally seen in mitral valve.
2D echocardiogram • Estimates the severity of MS • Measure the pressure gradient between LA to LV. • Define the etiology.
Surgery • Indications for intervention focus on: • Episode of pulmonary edema, • Decline in exercise capacity, • Evidence for pulmonary hypertension. • Percutaneous mitral balloon valvotomy: • Mitral valve area <1.5 cm2 • MVR: • Mitral valve area <1.0 cm2
Mitral Stenosis • Diagnosis & Differential diagnosis - Diastolic rumbling murmur at apex + X-film + ECG + Echo - relative MS; Austin-Flint murmur; left atrial myxoma ; Graham steell murmur • Complication: Atrial fibrillation; acute pulmonary edema; congestive heart failure; thromboembolism; infective endocarditis; pulmonary infective
Mitral Stenosis • Management: - Medical treatment: Antibiotics, Diuretics and Digitalis, Antiarrhythmic drugs, Anticoagulant - Percutaneous balloon mitral valvuloplasty ( PBMV) - Surgical treatment: Closed mitral valvotomy Open valvotomy Mitral valve replacement
Mitral Regurgitation • Etiology and Pathology - Abnormalities of valve leaflets: Rheumatic, infective - Abnormalities of the mitral annulus: dilatation, calcification - Abnormalities of the chordae tendineae: congenitally, infective, trauma, Rheumatic - Involvement of papillary muscle: CAD
Mitral Regurgitation • Pathophysiology In systolic period, blood flow from LV → LA, LA filling pressure↑; in diastolic period, LV accepts more blood →LV dilation, hypertrophy →LVEDP↑ →LAP↑→PCWP↑→PAP↑→RHF; CO↓ • Chronic • Acute
Mitral Regurgitation • Clinical Manifestations (1) Symptoms: asymptomatic( gradually,>20 years), palpitation, fatigue, dyspnea, pulmonary edema (2) Signs: - apical pulse→left,lower - apical beat heavy - cardiac dullness enlarged→left - pansystolic murmur at apex, radiate to left axilla, subscapular - S1↓,P2↑
ECG • Left axis deviation. • Left ventricular hypertrophy. • P waves broad, tall, or notched in standard leads. • Broad negative phase of diphasic P in V1.