Medicare Bad Debts
220 likes | 510 Views
Medicare Bad Debts. Overview of Medicare Policies. Agenda. Overview – What is a Medicare Bad Debt? Medicare Policies Requirements for Claiming Reimbursement from Medicare for Bad Debts Use of Collection Agencies Top 5 Bad Debt Mistakes Action Items Recent News Audits & Appeals.

Medicare Bad Debts
E N D
Presentation Transcript
Medicare Bad Debts Overview of Medicare Policies Presenters: Keith Williams & Associates, Inc. Kathy Whitmire, HTH Dale Gibson, Medicare Expert
Agenda • Overview – What is a Medicare Bad Debt? • Medicare Policies • Requirements for Claiming Reimbursement from Medicare for Bad Debts • Use of Collection Agencies • Top 5 Bad Debt Mistakes • Action Items • Recent News • Audits & Appeals Keith Williams & Associates, Inc.
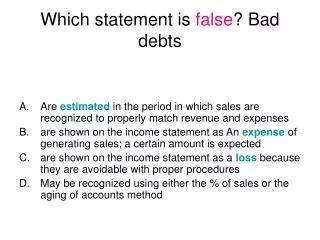
Medicare Bad Debts The Medicare Program was designed so that patients have amounts to be paid out of pocket in order for them to not abuse the program by over utilizing services. These amounts are known as the Patients Deductible and Co-Insurance. The amount that is due from the Patient for the deductible and co-insurance amount is subtracted from the Providers payment. Instead of the Medicare program bearing the responsibility for collecting these amounts it is the responsibility of the Provider to bill and collect these amounts from the patients. When Patients do not pay the Provider, the respective deductible or co-insurance amount this amount can then be determined to be a Medicare Bad Debt and reimbursable to the Provider if certain conditions are met.
Medicare Policies • Medicare Regulations state (42 CFR 413.89 (e)) the criteria for an allowable bad debt is: • The debt must be related to covered services and derived from deductible and coinsurance amounts. • The provider must be able to establish that reasonable collection efforts were made. • The debt was actually uncollectible when claimed as worthless. • Sound business judgment established that there was no likelihood of recovery at any time in the future. This is also found in the Provider Reimbursement Manual (PRM) 15-1 Section 308. Keith Williams & Associates, Inc.
Bad Debt Requirements • The debt must be related to covered services and derived from deductible and coinsurance amounts. • Hospitals can’t claim an amount for: • Non-Covered Services (Hospitals - CMS Publication 10 Section 260; Skilled Nursing Facilities – CMS Publication 12 Section 240) • Denied Claims – Only can claim for covered services and claims • Professional Fees – These services are not paid through the cost report and they are paid under by different part of the Medicare Program • Medicare Advantage/HMO Claims - These services are not paid through the cost report and they are paid under by different part of the Medicare Program. Providers should include language in their Medicare Advantage contracts to have these amounts recouped form the Plan. • Durable Medical Equipment - These services are not paid through the cost report and they are paid under by different part of the Medicare Program Keith Williams & Associates, Inc.
Bad Debt Requirements 2. The provider must be able to establish that reasonable collection efforts were made. • PRM 15-1 Section 310 Defines Reasonable Collection Effort as the following: “To be considered a reasonable collection effort, a provider's effort to collect Medicare deductible and coinsurance amountsmust be similar to the effort the provider puts forth to collect comparable amounts from non-Medicare patients. • It must involve the issuance of a bill on or shortly after discharge or death of the beneficiary to the party responsible for the patient's personal financial obligations. • It also includes other actions such as subsequent billings, collection letters and telephone calls or personal contacts with this party which constitute a genuine, rather than a token, collection effort. The provider's collection effort may include using or threatening to use court action to obtain payment.” Keith Williams & Associates, Inc.
Bad Debt Requirements 2. Continued • A provider's collection effort may include the use of a collection agency in addition to or in lieu of subsequent billings, follow-up letters, telephone and personal contacts. Where a collection agency is used, Medicare expects the provider to refer all uncollected patient charges of like amount to the agency without regard to class of patient. The "like amount" requirement may include uncollected charges above a specified minimum amount. • The provider's collection effort should be documented in the patient's file by copies of the bill(s), follow-up letters, reports of telephone and personal contact, etc. • If after reasonable and customary attempts to collect a bill, the debt remains unpaid more than 120 days from the date the first bill is mailed to the beneficiary, the debt may be deemed uncollectible. Keith Williams & Associates, Inc.
Bad Debt Requirements • 3. The debt was actually uncollectible when claimed as worthless. • If after the provider applies the “Reasonable Collection Efforts” in Requirement #2, the patient has not paid any or all of the amount owed the Hospital may claim the amount as a Medicare Bad Debt. • Actually Uncollectible When Claimed has evolved over the last 6 years. In 2005 Medicare began applying a “different” criteria to the uncollectible determination. In this change Medicare stated that it considers any collection effort whether by the Hospital or its Outside Collection Agency (OCA) to deem the account not worthless. • Why? It is Medicare’s opinion that any efforts to collect an account means the Hospital does not think the account is uncollectable. Keith Williams & Associates, Inc.
Bad Debt Requirements • 3. Continued. • In order to claim an amount on the Medicare Bad Debt report all collection efforts must cease. The account must be written off the Hospitals books and no further collection efforts made, even if the patient has future visits or services received from the Hospital. • All accounts must be returned at the same time from any OCA. (Hospitals can’t bring back Medicare accounts at 120 days and Commercial accounts at 180 days.) Keith Williams & Associates, Inc.
Bad Debt Requirements • Sound business judgment established that there was no likelihood of recovery at any time in the future. • Hospitals are not required to stop collection on accounts after 120 days. If a Hospital has determined that they can collect more money from all accounts if they try to collect them for 365 days then they can use this as their policy. • Sound Business Judgment means that the policies and procedures a Hospital uses in their collection efforts are thought out and planned accordingly. The Hospital must have a policy demonstrating it’s collection efforts and what it considers reasonable. If a Hospital changes its collection policy Medicare may require evidence to support the change that this is an appropriate change. Keith Williams & Associates, Inc.
Medicaid Crossover Claims • CMS issued Program Memorandum A-98-18, dated June 1998, indicating that in States where Medicaid does not fully pay for dual eligible beneficiaries’ deductible or coinsurance amounts providers may claim the difference as a bad debt for Medicare purposes. • Dual Eligible beneficiary is one that has Medicare as their primary coverage and Medicaid secondary. • FIRST, hospitals must bill the claim to Medicaid and have the “denial” to pay all of the deductible or coinsurance amount shown on a Medicaid remittance advice. • Once the State Medicaid agency has denied to pay 100% of the deductible or coinsurance amount it may be immediately claimed as a Medicare Bad Debt. There is no 120 day period since the patient is considered Indigent because they are qualified for Medicaid. • The Beneficiary must be qualified for and receiving Medicaid benefits during the stay or visit in order for the amount to be covered. Keith Williams & Associates, Inc.
Indigent Claims • The following guidelines should be used to determine if a Patient is Indigent (PRM 15-1 Section 312): • The patient's indigence must be determined by the provider, not by the patient; i.e., a patient's signed declaration of his inability to pay his medical bills cannot be considered proof of indigence. • The provider should take into account a patient's total resources which would include, but are not limited to, an analysis of assets (only those convertible to cash, and unnecessary for the patient's daily living), liabilities, and income and expenses. • The provider must determine that no source other than the patient would be legally responsible for the patient's medical bill; e.g., title XIX, local welfare agency and guardian. • The patient's file should contain documentation of the method by which indigence was determined in addition to all backup information to substantiate the determination. Keith Williams & Associates, Inc.
Indigent Claims • Continued • Once indigence is determined and the provider concludes that there had been no improvement in the beneficiary's financial condition, the debt may be deemed uncollectible without applying the “Reasonable Collection” Efforts under Section 310. • The debt can be claimed immediately on the Medicare Bad Debt Log. Charity determinations by the Hospital are not eligible to be claimed as a Medicare Bad Debt. • In most cases the Hospitals uses a % of the Federal Poverty Guidelines published annually to determine a Beneficiaries Indigency. Keith Williams & Associates, Inc.
Top 5 Medicare Bad Debt Mistakes • Failing to document collection efforts. • Failing to follow your own Policies on Collection Efforts. It is better not to have a policy than to have one and not follow it. • Not monitoring the OCA’s (Outside Collection Agencies) and how they are performing their collections. Also, failure not to monitor the accounts placed with the OCA’s. • Writing off accounts prior to the 120 day collection period and not proving the Beneficiary is Indigent. • Waiting to the last minute to try and complete the Medicare Bad Debt logs. Keith Williams & Associates, Inc.
ACTION STEPS: • Hospitals need to maintain and monitor their Medicare Bad Debts on a monthly basis. Weekly is my preferred method. Lot of Reimbursement at stake. • The Hospital should develop and maintain a system for tracking all claims sent to any OCA. • Hospitals should review their policies and collection efforts with each OCA used to be sure they understand your specific requirements. • Hospitals should write into their contracts with each OCA specifics on how each company is to work the accounts and that they will follow the Hospitals policies. Also, that they will indemnify the Hospital for their failure to follow the specific policies if Medicare denies the Bad Debt claim. Keith Williams & Associates, Inc.
ACTION STEPS: 4. Hospitals should have a contract with each Medicare Advantage/HMO stating they will reimburse the Hospital for each beneficiary Bad Debt claim. 5. Staff Education is the key to being successful in your Medicare Bad Debt reimbursement results. 6. Each Hospital Provider type should have it’s Bad Debt logged on separate logs; e.g. Inpatient, Outpatient, RHC, Swing Bed, Skilled Nursing, etc. • The Hospital should also maintain or specifically note on each log the accounts that are Crossover & Indigent Claims. • The CFO should remain transparent and keep the board apprised of discrepancies found in bad debt reporting. Keith Williams & Associates, Inc.
Recent Reduction in Bad Debt Reimbursement - 2/16/2012: According to the legislative language released today, cuts to hospitals to pay for the payment fix include: • Reductions in payments to acute care inpatient hospitals for assistance to low-income Medicare beneficiaries (bad debt) from the current 70 percent level to 65 percent in fiscal year (FY) 2013, • and from 100 percent to 65 percent over three years for critical access hospitals (88 percent in FY 2013, 76 percent in FY 2014, and 65 percent in FY 2015); • http://docs.house.gov/billsthisweek/20120213/CRPT-112hrpt-HR3630.pdf Keith Williams & Associates, Inc.
Documents: DOCUMENTS FOR TODAY’S BAD DEBT WEBINAR ARE ATTACHED • 1) CMS Compliant Bad Debt Log 2) Bad Debt Audit Checklist 3) CMS Bad Debt Policy and Procedure with detailed Instructions on how to comply • Important Links that will be referenced: • https://www.cms.gov/transmittals/downloads/R435PR1.pdf • http://dch.georgia.gov/vgn/images/portal/cit_1210/52/37/138800987CAHFiscalAnalysisPhase1.pdf • https://www.cms.gov/MLNMattersArticles/downloads/SE0824.pdf Keith Williams & Associates, Inc.
Audits & Appeals: Statistical Sampling Medicare Recoupment Process Extended Repayment Plan (ERP) Medicare Appeals Process Keith Williams & Associates, Inc.
Questions? Keith Williams & Associates, Inc.