Download
1 / 23
230 likes | 404 Views
Passing the Family Opportunity Act in North Dakota. Donene Feist Executive Director Family Voices – ND Edgeley, ND (pop. 562) HRSA/MCHB Partnership Meeting October 2007. North Dakota Gov. John Hoeven signed SB 2326. Sponsor: State Senators Tim Mathern and Dick Dever.

E N D
Passing the Family Opportunity Actin North Dakota Donene Feist Executive Director Family Voices – ND Edgeley, ND (pop. 562) HRSA/MCHB Partnership Meeting October 2007
North Dakota Gov. John Hoeven signed SB 2326. Sponsor: State Senators Tim Mathern and Dick Dever. Elizabethis the daughter of Roxanne Romanick, was involved in the legislation and was present at the ceremony. Photography by Shannon Wirrenga 1st in the countryFOA passed in ND, April 11, 2007
Financial Eligibility - 200% of the FPLNET(49,000 children >18*) Premiums- 5% of monthly Gross income Out of pocket expenses: child care costs, medical, taxes withheld, etc.) SAMPLE $ 41,300 Family of 4 (ave. ND annual income $53,323 **) $ 117 average estimated monthly premium Healthcare Benefits Analysis determines if current out-of-pocket expenses outweigh cost of buying into Medicaid. SOURCES: * 2007 Child Care in the State of: ND ** U.S. Census Bureau, CPS 2006 Annual Social and Economic Supplement The Outcome: FOA in ND
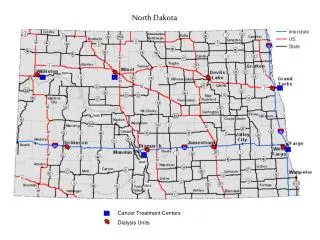
Nothing is Easy in ND • 70% of the 53 counties, are considered frontier only 13 cities have a population over 6,000 • Population density 9.3 persons per square mile US 79.6 persons per sq mile • Extreme weather 9 months of the year Contributes to isolation and travel difficulties Summer highs: 109 degrees heat indexes 125 degrees Winter lows: - 43 degrees wind chills of -100 degrees • ND residents embrace the tradition of the frontier spirit with great pride, dignity and passion.
ND Issues & Needs 74% Lack access basic health services SOURCE: Block Grant FY’2006 4-6 hr drive to “urban” areas for health care Bismarck(pop. 55,532)--or -- Fargo (pop. 90,599) Some go to the Twin-Cities in Minneapolis SSI does not mean automatic Medicaidin ND ND is a 209(b) state: CT, HI, IN, IL, MN, MO, ND, NH, OK, OH, VA) Requires separate Medicaid application, different requirements.
Prevalence rates are not significantly different from the national rates by age and gender. Source: DRC, 2006 CYSHCN in ND 12.4% 19,651 / 12.8% nationally 6.8% age 0 - 5 14.3% age 6 - 11 15.3% age 12 - 17 14.7% male 10.0% females
Underserved/Culturally Diverse 5 American Indian Reservations 2 Air Force Bases Religious communities -- Brethrens & Hutterites/German origin Large transient migrant population - agriculture Emerging immigrant population Kurdish, Arabic, Somali, Bosnian, and Vietnamese
ND Frontier Spirit: Proud & Stoic Labor Force working mothers - children ages 0-17 81.2 % vs national 69.1% / 2nd in the country (SD is #1) ND Kids Count, 2006 Families of CYSHCN 21.8% had to quit their job; not take a job or greatly change their job due to child care for their child. DRC 2001 Poverty 24 %Children live in poor and near poor families Over half of the ND 53 counties, Child poverty rate exceeds the state average of 16.8 percent ND KIDS COUNT 2006
Impact on Family Parents who have CYSHCNsaid …………. 30% Employment was affected most said they had given up a paying job, accepted a lower paying job with more flexibility or fewer demands, or had not changed jobs because the change leads to losing benefits. 60%missed one or more days of work due to their child’s special health care need 50% they had no paid sick leave or family leave
Why ND Needed FOA: Data on of CYSHCN 31.0% have public insurance SCHIP is not adequate 12.9% have had no insurance in the last 12 months 19.1% needed special services, equipment or other 24.0% Families experience financial problems due to child’s health needs 22.0% Families not able to pay for financial costs for their child’s health care needs. - 66% paid out of pocket expenses. - 40% amount for out of pocket was a financial burden DRC: 2001
What Would it Take to Get FOA passed? • Education– Getting others interested (Family Leaders, Consumers, Families, Providers, Legislators, Media) • Partnerships – Joining forces Department of Human Services ie: Medical Services Division, Children’s Special Health Services, North Dakota Disabilities Advocacy Consortium, Children’s Caucus, Family Voices of ND, Protection and Advocacy workgroupwhich included advocacy groups • Bill sponsors– Bipartisan/Senators Fischer, Lee and Mathern, Representative Price and Schneider • Department Buy-In: Medicaid had heard much about the FOA through many avenues and through interim legislative committee as did many of the legislators. Department of Human Services instrumental in OAR. Medical Needs Task Force met before session which helped get folks “on the same page” • Staying on the Radar– public, families, legislators
Previous Legislation that Sets the Stage - 01 2003 Home & Community Based Services HB 1148: Relating to personal care services for eligible medical assistance recipients who are residing in their own homes; and makes permanent the personal care option for individuals eligible for the Medicaid Program. It required the department to submit a waiver that would permit disabled and elderly individuals to direct their own care. (Passed)
Previous Legislation that Sets the Stage - 02 2005 • HCR 3054: A concurrent resolution directing the Legislative Council to study state programs providing services to children with special health care needs to determine whether the programs are effective 2005 • Senate Bill No. 2395. Bill created a program for children with Russell Silver Syndrome and directed the DHS to apply for a waiver to provide in-home services to children with extraordinary medical needs who otherwise require hospitalization or nursing facility care.
Education & Information: Not Lobbying Making the Case using State Data - Insurance - Chart Book, 2006, Catalyst Center - National CSHCN Survey, 2001, Data Resource Center - Needs Assessment for proposed waiver, Medical Needs Task Force, Dept. of Human Services/Private insurance 2006 - Family Unmet Needs and Costs, FV-ND Survey, 2006
Education & Information: Not Lobbying Educating through Information – packets & emails - Fact sheets (easy to read and understand one pagers) - Family Stories (booklet w/pics, putting a face to the issue) - Promotional materials (events, resources for addl info) - Informational alerts (email, fast track, calls/visits to State House) - Testimonies (organized and not duplicative)
The Roller Coaster Ride: Ups & Downs December/ 2006Governor OAR list December 2006-January 2007 Bill sponsors January 22 2007Senate testimonies, media blitz February 9, 2007Passed in the Senate February 2007-March 2007House complicated March 8, 2007Bill in trouble March 2007Families rallied, sent letters, made calls, walked halls Jan-March 2007Alert statewide/providers, families March 29, 2007The Vote
Blood, Sweat & Tears: Winning & Compromising OUTCOME:Bill passed and signed, April 11, 2007 - 200% of FPL (family leaders had hoped for 300 FPL) • $ for waiver in addition to the Medicaid Buy-In included in the FOA Bill • Monitoring Needed: Tracking of denials and income • Education & Outreach maximized thru Partnerships • On-going education - Grassroots/families (about the program, application process and paperwork)
Advice with Hindsight: Tips for Title V Leaders Consumer Leadership Organizations are Allies • Conduct Annual Needs Assessment - checking the pulse at the community level (tracking intake calls/emails) - Access to families at the Community Level -Informed consumers are terrific allies (freedom of speech-no job jeopardy) • Keeping a Face to the Issue - Short IMPACT stories with pictures - Capture ROI (return on investment) model. ie. Families can pay taxes
Other Implementation Considerations • FTE may be needed • It takes time to hire and train staff meanwhile others carry the work load • Need to add new eligibility group so changes required to the state MMIS system • Multiple competing issues after a session can make implementation difficult, can mean some lag time. • Ongoing communication needs to transpire with family organizations and among staff before, during and after implementation to assure everything is working properly
Family Voices of ND Donene Feist Executive Director fvnd@drtel.net / www.fvnd.org 701-493-2634