Download
1 / 28
280 likes | 716 Views
Medicare Part C and the CMS- HCCs. Gail Woytek, RHIA , CCS June 2, 2014. AGENDA. What is Medicare Part C? What is Risk Adjustment? Who is being Risk Adjusted? How are they being Risk Adjusted? What is an HCC? How does HCC coding differ from inpatient or outpatient coding?

E N D
Medicare Part C and the CMS- HCCs Gail Woytek, RHIA, CCS June 2, 2014
AGENDA • What is Medicare Part C? • What is Risk Adjustment? • Who is being Risk Adjusted? • How are they being Risk Adjusted? • What is an HCC? • How does HCC coding differ from inpatient or outpatient coding? • What is a RADV audit?
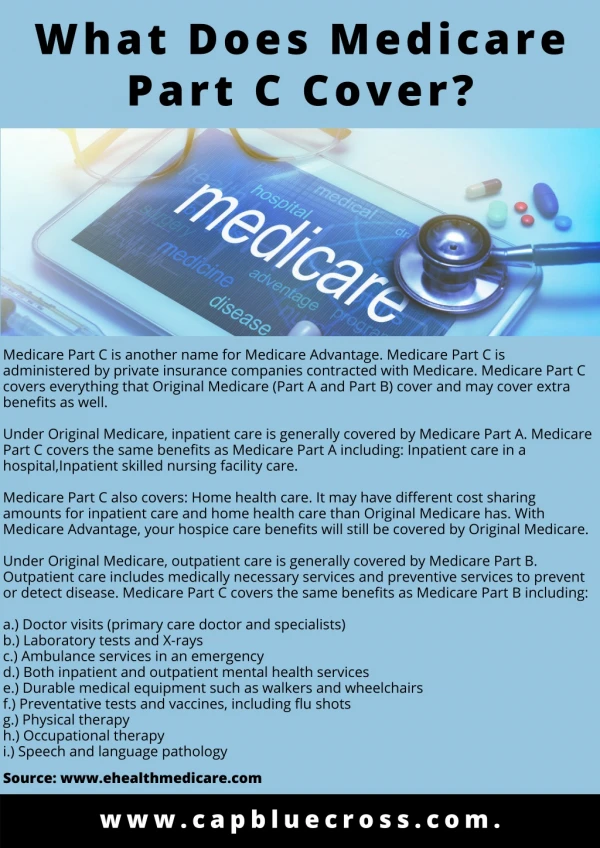
Medicare Part C Called Medicare Advantage Plans These are similar to private health plans and take the place of “Original Medicare”. These plans must be approved by Medicare and follow Medicare rules, Medicare pays a fixed amount each month to the company offering the MA plan.
What is Risk Adjustment? • The process of accommodating chronic conditions to determine the amount of reimbursement to the health plans • It is used to determine the clinical acuity of patients, the diagnostic profile • It can be done prospectively, concurrently and retrospectively
What is Risk Adjustment cont. • Risk Adjustment allows CMS to pay plans for the risk of the beneficiaries allowing Medicare to make appropriate and accurate payments for enrollees with differences in expected costs. • 100% risk adjusted payment for MA plans completed in 2007,began in 2004
Who is being Risk Adjusted? • Those participants eligible for Medicare • Dual eligible special needs patients that are entitled to medical assistance under a Medicaid state plan. Medicaid Managed Care • Can be on or off the Health Insurance Exchange • ESRD patients • Accountable Care Organizations
PACE Programs • Program for All inclusive Care of the Elderly • Risk score based on a participant’s demographic factors and diagnoses codes • A frailty factor is also used to determine Medicare payment. Frailty factors are based on the number of limitations in activities of daily living
How are patients Risk Adjusted? Payment is based on the expected health care costs using diagnoses from the previous year and this demographic data: Age, Sex, Medicaid Status, Original reason for entitlement, institutionalized and fraility
Prospective Risk Adjustment • Coding diagnoses from a Health Risk Assessment tool In Home visit, or with PCP Covers HCC and non HCC dx and Hedis review measures • Annual wellness visit
Concurrent/Retrospective • Clinical Reviewers on site • Paper copies faxed, mailed • PDFs • EMR on site or remote access
What is CMS HCC? Hierarchical Condition Category • Essentially a category of ICD-9 codes that fall in to a related disease process or condition • There are also RX-HCCs • Not all codes fall in to an HCC
CMS-HCC Model Table • The Risk Adjustment models change each year • Payments differ between MA models and PACE models • This year there is a blended model for MA plans to determine risk scores
HCC Payment values • The lower the HCC number, the higher the acuity and therefore payment • PACE and ERSD use same model • Some HCCs “trump” others
What codes to capture? • For HCC coding not all codes fall in to an HCC and would therefore not be submitted for example: HTN, Asthma, hyperlipidemia • “History of” codes do not “count” • DO code ongoing chronic conditions that are being treated such as: DM, COPD, CHF
ACCEPTABLE DOCUMENTATION • Face to face visits for the review year! • Legible • Signed • Clear, consistent, complete documentation • Acceptable provider types • MDs and extenders • PT, OT
Clear and Concise! • “the interpreter speaks her diuretic” • “Pt wants red string on her pessary, it is symbol of good luck and the color of fire will scare away evil” • Social History: “He was fishing all day today and caught a few fish” • “knot behind R ear/ knot behind knee” • “breasts continue to be pendulous”
Acceptable, cont. • Acceptable Facilities • Acute Care • Religious health care institutions
Benchmark Dx/ Target Dx • Benchmark data is based on the dx codes submitted the year before, PCP offices, hospitals, consultants • Target dx are those that informatics may determine would logically be present, but not captured • Other conditions that are being monitored, evaluated, assessed, treated
ADDENDS • Similar to physician inquiries • Missed opportunities: • Chronic conditions such as renal disease are not listed as chronic • Chronic diseases that are (MEAT) need to be documented at least once each payment year • Highest degree of specificity not documented
Coding Guidelines • Outpatient guidelines are used; cannot use “suspected”, “probable” • Cannot code directly from a diagnostic test, the PCP must verify the diagnosis • Must code from the exact narrative documented by the provider and not make assumptions • Only code to the highest degree of specificity
RADV Audits • RISK ADJUSTMENT DATA VALIDATION • Annual audits conducted by CMS to verify plan’s risk adjustment payments • National: Several plans asked to submit a small sample documentation, with no financial implications • Targeted: 30 plans, both MA and PACE per review year with financial implications
RADV Audits, cont. • CMS goals of these audits are to determine the national payment error rate for MA programs and to assess the quality of the data submitted for payment • Enrollee based stratification, those with highest risk scores, lowest risk scores and the middle stratum, this reduces the variability that a random sample would have
QUESTIONS? • Thank You!!