Download

1 / 32
320 likes | 415 Views
Explore the variations in emergency medical services protocols and education between Australia and Taiwan, highlighting scope of practice, drug administration, and historical context. Identify challenges, strengths, weaknesses, and opportunities for improvement in EMS delivery. Investigate similarities between prehospital and emergency department settings. 8 Relevant

E N D
Emergency Medical Services guideline differences between Australia and Taiwan Dr Jason C BendallMStJ AdvDipParamedSc(Ambulance) BMedSc(Hons) MBBS MM(ClinEpi) PhD FACAPFPA www.drjasonbendall.wordpress.com
Key Facts Australia Taiwan 35,883km2 (137th) 23.17 million • 7,741,000 km² (6th) • 22.62 million
EMSin Australia • State based Ambulance Services • Government funded • Majority government run • Majority aligned with Ministries of Health rather than Emergency Services • Private ambulance services exist (not triple zero) • Non-emergency patient transport • Remote / Mining locations • Event “first aid” sector • No direct medical control (protocols / guidelines) • Non-transport rate ~20%-25% • Computer aided dispatch
Training / Education • Transitioning to higher education sector • “Graduate” paramedics with 3 year bachelors degree (some accelerated programs) • Not yet able to reliably meet all of industry needs • Graduates not “work ready” at graduation • Require internship / supervised practice (~12 months) • Some vocational “in house” training • Diploma Paramedical Science (Ambulance) • Advanced Diploma Paramedical Science • Takes 3 years to become qualified
Scope of practice– “paramedics” Varies between jurisdictions but typically: • Skills • Airway: OPA, NPA, LMA, suction • Breathing: BMV, oxygen therapy • Circulation: IV access + IVF • Defibrillation • Monitoring: HR, RR, BP, SpO2, ECG • Diagnostics: BGL, 12 lead ECG • First aid, collars, splints, pelvic binding, extrication
Scope of practice – “paramedics” • Drugs: • Aspirin / Glyceryltrinitate (ACS) • Glucose gel / Glucagon / Dextrose (hypoglycaemia) • Adrenaline i.m.(anaphylaxis / asthma*) • Adrenaline i.v. (cardiac arrest*) • Salbutmaolnebules / Ipratropium bromide (Asthma / COPD) • Methoxyflurane / Morphine / Fentanyl(Pain) • Ondansetron / Metoclopramide (Antiemetics) • Midazolam (seizures) • Naloxone • Benzylpenicillin / Ceftriaxone • New areas of practice include prehospitalthrombolysis and assessment / management low acuity patients
Sample clinical practice guidelines http://www.ambulance.vic.gov.au/Media/docs/x01_CPG_ADULT-web-835ff459-ac3e-454e-880b-0fac0c92c212-0.pdf
History of Intensive Care Paramedics • Introduced at time when “paramedics” had very limited scope of practice • First models in 1970s • Concept – cardiac care out of hospital • Management of cardiac arrest • intubation / ACLS • Management of trauma (IV access / fluids) • Training in hospital / on road ~ 6 months
Scope change over time % of maximum current scope of practice of ICP
Intensive Care Paramedics • Varies between jurisdictions, typically: • ACLS (adrenaline, amiodarone, atropine) • Frusemide • Sodium bicarbonate • Calcium gluconate / Magnesium chloride • Hydrocortisone / Dexamethasone • Endotrachael intubation (non-drug assisted) • Decompression of tension pneumothorax • Some include: • RSI (fentanyl / midazolam / suxamethonium ) • Ketamine • Adenosine / Metaraminol / Metoprolol / Noradrenaline • Pacing / synchronised cardioversion
EMS Taiwan Australia Began late 1890s Formal education 1961 EM recognised specialty 1993 ICP training 1976 • Began in 1960s • Formal EMT curriculum 1990s • EM recognised specialty 1998 • EMT-P training 2002
Challenges for all EMS providers • Rising demand for services • Aging population • Increasingly complex health care needs • Consumer expectations • Spectrum of acuity in case mix • Diversity of communities in metropolitan, regional and rural locations
Strengths • Scope of practice for majority EMS workforce meets the clinical need for the majority of acute presentations • Standard of care is essentially standardised • Progressive strategies for trauma, cardiac and stroke care • Increasing use of electronic medical records • Comprehensive and integrated HEMS / medical retrieval systems • Strong clinical governance practices • National Registration expected in 2014
Weaknesses • Accessing clinical placements is difficult for students • Curriculum still focuses on meeting acute care needs • Slow to implement changes to evidence • Innovation is variable across jurisdictions • Over emphasis on operational performance measures • Limited access to continuing professional development once trained
Opportunities • Development of “Extended Care” scope of practice to meet the needs of patients who do not necessarily require transport to ED • Development of community paramedicine and community paramedics in rural and remote areas • Research to minimise the gaps in EMS knowledge
How similar is the prehospital setting to the emergency department? • For all transported patients: • Same acuity • Same case mix • Same demand pressures • Opportunity to derive patient outcomes • Opportunity for passive learning • Opportunity for structured teaching • Access to many inter-professional mentors • Patient’s have plenty of time • Plus….australian paramedics spend a lot of time in ED…. opportunity for informal teaching?
Paramedic roles….how different from emergency physician roles? Communicator Collaborator Manager Health advocate Scholar Professional Medical expert integrating the above competencies in clinical practice • Medical expert with regard to the knowledge, skills and attitudes required in the specialty for the appropriate assessment (history, examination, investigation), diagnosis and management (supportive care, specific care and disposition) decisions involved in patient care • Medical expert with regard to the procedural and technical skills required in the specialty
What is possible? • Extended Care Paramedics • Qualified paramedics • 10 weeks additional training (380 hours) • Clinical school setting • Focus on minor illness / minor injury (patients who could potentially be treated outside ED) • Clinical decision making / risk management • Patient assessment and history taking • Scope includes suturing, reduction of dislocations, antibiotics, insertion of IDC, antibiotics, oral analgesics (including oxycodone), plastering, falls assessment, aged care assessment • Associated with increased odds non-transport
Paramedics are highly capable • Dependent on education, training and experience • Dependent on medical leadership • Solution to many health gaps • Can work in and across traditional boundaries • Well placed to contribute positively to the health of their patients • Unable to self determine scope of practice
Barriers to progress • Patient expectations • Community expectations • Evidence (lack of) • Patient safety • Economics • Politics • Workforce expectations • Leadership • Legislation / legal
Drivers of scope of practice • Patient needs (expectations) • Community needs (expectations) • Evidence • Patient safety • Economics • Politics • Workforce needs (expectations) • Leadership
Model for EMS PARAMEIDC PROFESSION PARAMEDICS PATIENTS
Fundamentals of EMS education • Recognition and management of cardiac arrest • Primary assessment (ABCDE) • Including measurement of vital signs • History taking • Patient assessment • Medical • Trauma • Focussed diagnostic tests • Clinical decision making • Clinical risk management • Developing skills in the assessment and management of low acuity problems • Specific managements based on best available evidence
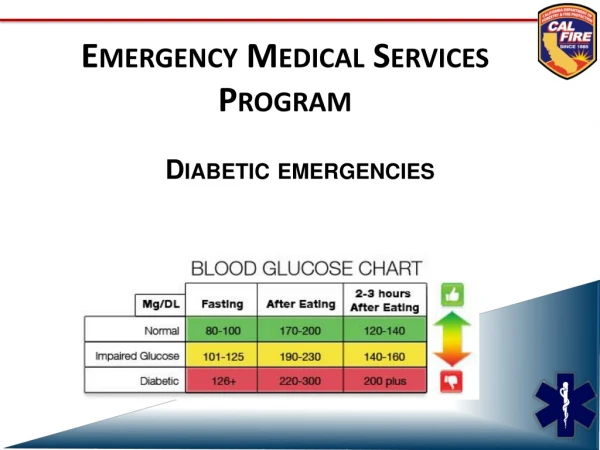
Scope goals for modern EMS • Assessment and management of: • Cardiac arrest • Recognition, quality of CPR, defibrillation, outcomes • Recognition of at risk and deteriorating patients • Vital signs recording, interpretation, monitoring standards • Treat acute pain • Treat reversible / life threatening conditions • Hypoglycaemia, asthma, anaphylaxis, sepsis, COPD, seizures • Cardiovascular emergencies • ACS, dysrhythmias, CCF, stroke • Trauma • Aware of patient outcomes (especially non-transported patients)
Strengths • New and developing EMS • Training time • EMT 1 40 hrs • EMT 280 hrs • EMT-P 1280 hrs + hospital based • Essentially one EMS • Not too small – not too large
Opportunities • Improved pain management • Intranasal drug delivery • Fentanyl, midazolam, ketamine, ? glucagon • Early intervention for acute emergencies • Anaphylaxis, asthma, seizures • Developing stronger quality improvement and patient safety systems – developing a just culture • EMS research
But we’re so close to a hospital…. • Patients get sick of where they get sick • Emergency care should start at the scene not at the ED • The prehospital setting is an extension of the ED • In my experience a patient is never just 5 minutes from the ED: • Time to assess • Time to treat • Time to load • Time to drive • Time to unload • Time to be triaged • Time to off-load
EMS interventions now in the Australian community • AED for SCD • Aspirin for ACS • Oral glucose and glucagon for hypoglycaemia • Adrenaline auto injectors for anaphylaxis • Salbutamol for asthma • Methoxyflurane for pain
Better standards Better paramedics Better care drjasonbendall.wordpress.com | drjasonbendall@gmail.com