Download
1 / 44
440 likes | 711 Views
Presented by Ahmed Walid Anwar Morad, M.D Assistant Professor of Obstetrics and Gynecology Banha Faculty of Medicine Egypt 2013. Intrauterine Insemination for Unexplained Infertility. OBJECTIVES.

E N D
Presented by Ahmed Walid Anwar Morad, M.D Assistant Professor of Obstetrics and Gynecology Banha Faculty of Medicine Egypt 2013 Intrauterine Insemination for Unexplained Infertility
OBJECTIVES The main objective of this presentation is to spotlight on the role of IUI in the treatment of unexplained infertility
Definition Unexplained infertility means that ,couple does not conceived after 1 year of unprotected vaginal sexual intercourse, with basic infertility evaluation shows no obvious abnormality (RCOG guidelines,1998; Randolph,2000; ASRM,2006). Incidence 15% to 30% of infertile couples (ASRM,2006)
Basic investigations for diagnosis of Unexplained infertility Normal basic semen analysis according to WHO criteria (WHO ,2010). Patent fallopian tube confirmed by HSG. Ovulation confirmed by mid-luteal serum progesterone level.
In unexplained infertility: the cause is not defined ,so the treatment is empirical (ASRM, 2006). Expectant Encourage Advice Inform Active IUI Oral stimulating agents (CC / letrozole) CC+ IUI Gonadotropin injections with or without IUI IVF/ICSI Alternatives: Bromocriptine, Danazol, Tubal flushing.
Treatment Dependent on: Availability of resources , Patients’ age , Duration of infertility. The standard protocol is to: Progress from simple to complex treatment options, Balance the effectiveness against the cost and side effects. (Ray et al,2012)
Suggested Protocol for Management of Unexplained Infertility (Ray et al, 2012)
IUI • Definition • Rationale • Other indications of IUI • Steps • Advantages • Complications • Indications of IUI in unexplained infertility • Effectiveness of IUI in unexplained infertility
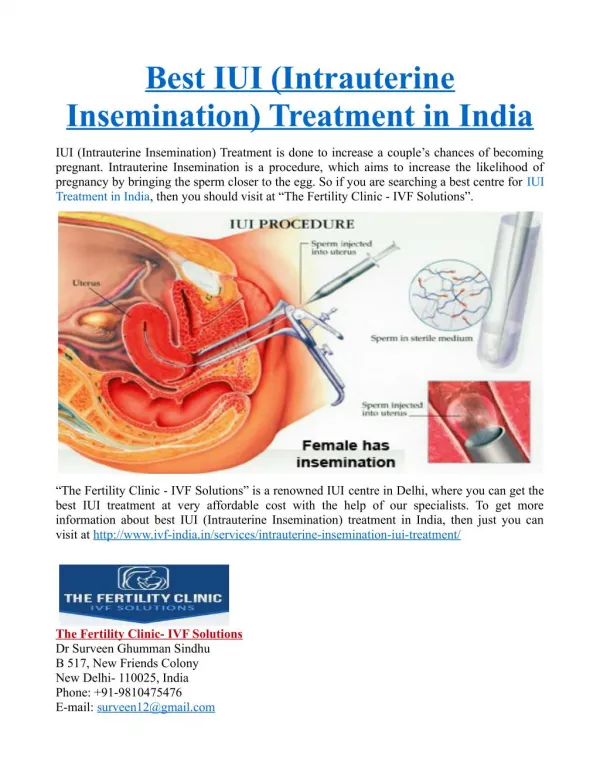
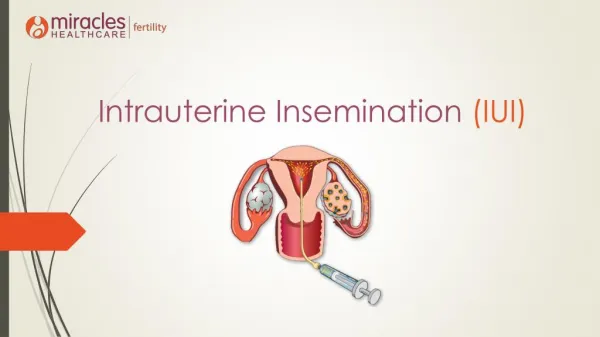
Intrauterine Insemination Definition IUIinvolves the placement of processed semen into the uterine cavity around the time of ovulation (Allahbadia and Merchant,2012).
Rationale increase the rate of conception by increasing the chance that maximum number of healthy sperms reaches the site of fertilization(ESHRE,2009).
Indications I. Male: 1. Ejaculatory failure: ( sever hypospadius ;retrograde ejaculation; impotence) 2. Male factor infertility (mild ;moderate) 3. Sperm cryopreservation prior to treatment ofhusband cancer. 4. Processed semen of HIV + husband for HIV negative women(NICE, 2013)
II. Female: 1.Cervical factor infertility 2. Endometriosis 3. Ovulatory dysfunction 4. Combined non-tubal infertility factors III. Combined: 1.Unexplained infertility • 2. Immunological infertility
Steps Patient selection & counseling. Natural cycle IUI Stimulated cycle IUI (Ovarian stimulation) Monitoring of treatment Sperm preparation Insemination
Advantages of IUI Non invasive (like Pap smear). Bypasspossible cervical mucous hostility. Easy:performance and training Minimal: cost and risk
IUI Complications Of the procedure Infection Pain Psychological(guilt, anger, loss of self esteem) Of COH Multiple pregnancy OHSS Antenatal & perinatal As pregnancies from sexual intercourse.
ESHRE Capri Workshop Group (2009) IUI or stimulated ovary/IUI is indicated as empiric treatment for all categories of unexplained infertility 20% of couples after initial work-up. Couples with mild male subfertility (20–40%) 50% of those in whom conventional treatments have failed.
NICE Guidance Feb, 2013 In the treatment of unexplained infertility The evidence does not support the use of IUI as an alternative to expectant management . IUI (with or without stimulation) should not be routinely offered (exceptions e.g. when people have social, cultural or religious objections to IVF)
Effectiveness of IUI in treatment of unexplained infertility
(Guzick et al. 1998.) Conclusions (Cochrane, 2012 ) : In stimulated cycles PR was higher with IUI compared to timed intercourse Unexplained Infertility : PR with different treatment Options
NICE Guidance Feb, 2004 ; For unexplained infertility ovarian stimulation should not be offered, even though it is associated with higher pregnancy rates than unstimulated IUI, because it carries a risk of multiple pregnancy. Cochrane, 2012 ; risks and alternative treatment options of stimulated IUI should be discussed. NICE Guidance Feb, 2013 ; Do not offer oral ovarian stimulation agents (such as clomifene citrate, anastrozole or letrozole) to women with unexplained infertility.
IUI versus alternative insemination techniques 1 } Fallopian Tube Sperm Perfusion (FSP) : Past : FSP is superior to IUI (Trout & Kemmann,1999) . Later: a meta-analysis reported no clear benefit (Cantineau et al, 2009) 2}No difference between IUI andIntraperitoneal insemination (IPI)(Noci et al,2007) 3}Intrauterine tuboperitoneal insemination (IUTPI) is superior to IUI &FSP (CPR/cycle 29.4% ) (Mamas, 2006) 4}IUI is superior to Intracervical insemination ICI(Besselink et al,2008).
IUI Vs. IVF for unexplained infertility Starting treatment with IUI rather than IVF was either cheaper or more cost-effective than IVF in unexplained infertility (Goverde et al., 2000). Cochrane, 2012(Pandian et al, 2012) IVF may be more effective than IUI+SO. Due to lack of data from RCTs the effectiveness of IVF for unexplained infertility relative to expectant management, clomiphene citrate and IUI alone remains unproven.
For people with: unexplained infertility, mild endometriosis or mild male factor infertility, who are having regular unprotected sexual intercourse: advise them to try to conceive for a total of 2 years before IVF will be considered . • NICE Guidance Feb, 2013
IUI in stimulated cycles may be considered while waiting for IVF or when in women with patent tubes, IVF is not affordable (ESHRE Capri Workshop Group, 2009)
Favorable Predictors of IUI Outcome Factors related to couples Factors related to therapy
Couple: • 1.Female age≤ 35y (Morshedi et al, 2003 ) • 2.Shorter duration of infertility . • 3. Type of infertility (Guven et al,2008)
Couple: • 4. First treatment cycles (≤ 4). • Pregnancies resulting from IUI occur during the first 3-4 treatment cycles (88-95.5%; respectively) • (Morshedi et al,2003). • Aboulghar et al, 2001, suggested a maximum of 3 COH/IUI cycles for treatment of unexplained infertility • However ,others recommended up to 6 cycles • (Dickey et al, 2002; Morshedi et al,2003; Ray et al, 2012).
5. Cause of infertility: (Bourn Hall clinic, 1999 ;Tay et al,2007; Wang et al,2008). Overall CPRs/cycle Higher PR with : Unexplained infertility (9.2% to 22% ) Ovulatory dysfunction (19.2%) Modest PR→ Cervical factor (16.4%) Poor PR: Endometriosis (11.9%) Immunological infertility (10% ) ♂ factor→ the best PR with ejaculatory disorders (13.3%)
B. Therapy:(Allahbadia and Merchant,2012). 1. Use of CC/HMG-FSH compared with CC only . 2. Follicular dynamic : - AFC > 5 (Ombelet et al, 2003) - Preovulatory follicles : 2–3 follicles≥ 16 mm with uniformly high-grade vascularity and E2 levels >500 pg/mL on the day of hCG administration. (Steures et al, 2004; Bhal et al ,2001) .
.3. Sperm parameters: generally • Processed total motile sperm count ≥ 10 million, 24 h survival > 70%, and normal sperm morphology of >4% (according to Kruger’s criteria) predict pregnancy outcome with 94% sensitivity, 86% specificity (Guven et al, 2008;Abdelkader & Yeh ,2009).(12.3 vs 2.8%) • Initial sperm count, motility ?
4.Time of insemination, preferably between D13 &16. 5. Endometrium: adequate thickness with trilaminar pattern (Tomlinson et al ,1996)
Measures does not affect IUI results 1. US monitoring & HCG induction of ovulation versus urinary LH monitoring of ovulation. HCG allow final follicular maturation (Kosmas et al, 2007) 2. GnRH agonist and antagonist. ↑complications (Allahbadia and Merchant,2012). 3. Double IUI versus single IUI (Polyzos et al,2009).
4. Type of catheter:no significant difference in PR when usingthe softer Wallace catheter or the less pliable Tomcat catheter during IUI, with the standard gentle non touch technique (Smith et al,2002). However , Merviel et al ,2010 recommended soft catheter. 5 . Luteal phase support do not appear major requirements in IUI cycles (ESHRE ,2009) 6. Sperm preparation technique (ESHRE,2009).
How to improve IUI results?Measures to↓ complications: 1. Natural cycle IUI: ↓ PR 2. Mild ovarian stimulation : low dose GnH 3. Cycle cancellation {> 3 follicles ≥ 16mm or; > 8 follicles ≥ 12mm} 4. Selective follicular reduction. (not routine) 4. Conversion to IVF cycle
How to improve IUI results?Measures to↑ PR: 1. COH: all except sever male factor ( Risks???) (Cohlen,2002). 2. Vaginal misoprostol.???? (Brown et al,2001; Barroso et al,2001). 3. 10 -15minutes bed rest after IUI (Saleh et al,2000 ; Custers et al, 2009 ) 4. Cervical mucous aspiration before IUI (Paasch et al, 2007)
5. Timed intercourse within 12 -18 h period: useful in IUI with low number of motile sperm inseminated (Huang et al, 1998). 6.Postponing IUI until the observation of follicle rupture by TV sonography ( PR;25% vs 8.8%) (Kucuk ,2008). 7. US guidance in IUI (Ramón et al,2009; Oztekin et al,2013) 8. Pre-insemination hydrotubation (Edelstam et al, 2008; Aboulghar et al, 2010 ; Morad & Abdelhamid , 2012)
Conclusions • Treatment of unexplained infertility is empiric as no obvious abnormality was detected. • Treatment of unexplained infertility is very much dependent on availability of resources and patients’ age and duration of infertility . • OH with IUI is a simple ,cost-effective, least invasive first-line treatment for Unexplained infertility.
Conclusions 4.Couples should be fully informed about the risks of IUI and COH as well as alternative treatment options. 5. In unexplained infertility OH with IUI may be considered while waiting for IVF or when IVF is not affordable. 6. The pregnancy rates of FSP & Standard IUI are similar.
Conclusions • 7.Pre-insemination hydrotubation, US guided IUI , cervical mucous aspiration, post-insemination bed rest for 10 min and vaginal misopristol may improve IUI outcome . • 8. In unexplained infertility, up to 6 cycles of IUI should be considered before shifting to IVF.
Thank you E.mail:::ahwalid2004@yahoo.com