Download
1 / 17
180 likes | 531 Views
Undernourishment and Child Malnutrition in Asia. S. Mahendra Dev Director, Centre for Economic and Social Studies, Hyderabad, India. Contents. Dimensions What are the reasons for high levels of Undernourishment and Child Malnutrition?

E N D
Undernourishment and Child Malnutrition in Asia S. Mahendra Dev Director, Centre for Economic and Social Studies, Hyderabad, India
Contents • Dimensions • What are the reasons for high levels of Undernourishment and Child Malnutrition? • What are the policies and actions needed to reduce them? (Including best practices) • We concentrate more on child malnutrition because it reflects the status of adults also particularly women’s health and well being.
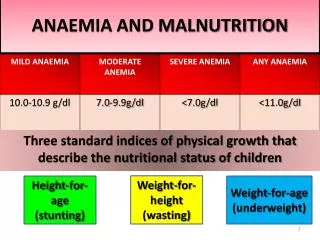
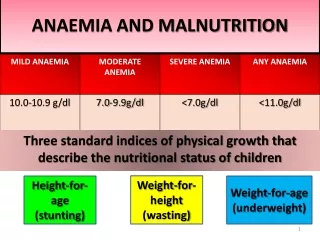
Dimensions • Two measures of Hunger under MDGs: • One measure is undernourishment : the proportion of people consuming less than the minimum dietary requirement (suffer from hunger) • Another measure is Child malnutrition or undernutrition : Weight for age • FAO data on undernourishment : 820 million undernourished in developing countries: 524 million in Asia • The undernourishment rate declined from 20% in 1990-92 to 16% in 2001-03. The decline was mainly due to China from 194 to 150 million. • India has the largest number in the world. Declined marginally from 215 to 212 million in one decade.
Dimensions • The number in DPR Korea doubled from 3.6 to 7.9 million. In Tajikistan prevalence was 60%. • The more important indicator of hunger is Child Malnutrition (underweight: weight for age) • Levels of child malnutrition is exceptionally high in South Asia. 45% to 48% of Children in India, Bangladesh and Nepal suffer from underweight. • It is 38% in Pakistan, 30% in Sri Lanka. • These numbers are much lower for other countries – 28% in Sub-Saharan Africa and 8% in China. • Many of the Asian countries may achieve MDG in income poverty but not in undernourishment and child malnutrition.
What are the Reasons for High Levels of Undernourishment and Child Malnutrition? • Low per capita income. Cross-section data –the percentage decline in malnutrition is roughly half the rate at which GNP per capita grows. • Thus economic growth alone can not reduce malnutrition. For example, in India, GDP growth was 6 to 7% per annum during 1992-93 to 2005-06. • But child malnutrition declined from 52% to 47% --0.5 percentage points per annum. • In fact, the per cent of underweight children in India declined only one percentage point from 47% in 1998-99 to 46% in 2005-06 inspite of high economic growth.
Reasons for high Levels • Income poverty is another reason. • However, studies have shown that malnutrition exists even after removal of poverty. • For example income poverty in India is 26% while child malnutrition is 46%. • The data for India, Bangladesh and some other countries show that malnutrition levels are surprisingly high even in rich income quintiles. • Thus, reduction in malnutrition is going to be a bigger challenge than income poverty.
Reasons for high Levels • Therefore, one has to look beyond economic growth, income poverty and food availability • Adequate nutrition during pregnancy and first six months of life are critical because of the impact on birth weight. • Thus, the problems often start before, during and after pregnancy as malnourished mothers are more likely to produce low birth weight babies. • Poor nutritional status at birth is perpetuated by inadequate breastfeeding and supplementary feeding habits. • Subsequently in the first two years, they do not give sufficient quality food –particularly mothers with low education.
Reasons for High Levels • Similarly, public health services are poor in South Asian countries. • Health sector performance in some of the Asian countries show that there are basically six problems --low levels of health indicators --slow progress in these indicators --significant regional, social and gender disparities --poor quality delivery systems in health --privatization of health services • Low standards of health and hygeine play important part since sick children are able to absorb essential nutrients.
Reasons for high levels • Micro nutrient deficincy is another reason • Age-specific interventions upto five years are important. But, lack of institutional arrangements for age-specific nutritional programs is another problem. • To conclude, there is a strong association between child malnutrition and women’s health/well being. • For example, one third of Indian women suffer from Chronic Energy Deficiency and BMI of less than 18.5kg • 58% of pregnant women in India suffer from anaemia • About 68% of pregnant women make first ANC visit after 4th Month of pregnancy. • One third of them visit after sixth month of pregnancy • About half of the deliveries take place at home
What are the Policies and Actions Needed? • Economic Growth: Inclusive, broad based, pro-poor • Agriculture and Rural Transformation: Through agricultural diversification and promotion of rural non-farm sector can improve productive employment • Small and marginal farmers should diversify. This can increase purchasing power and reduce undernourishment. • Food and nutri. security does not mean ‘foodgrain’ security • China offers many lessons for rural transformation • Urbanization: Urban areas also have high levels of child malnutrition. • Urban outcomes in metropolitan areas are poorer than rural in some countries (e.g. Bangladesh). Therefore, special challenges posed by urban areas must be addressed.
Policies and Actions • Sector Specific Policies: Economic growth is not enough. Sector specific policies are needed. • For example, a package consisting of expanded child and maternal immunization, antenatal care coverage, • nutritional supplementation (including breast feeding) and home based neo-natal services (including treatment of pneumonia) bring about significant reduction in both infant mortality and child malnutrition . • In other words, basic health services have to be improved. • Women’s Health and Well Being: Malnutrition can be reduced by enhancing women’s health, promoting gender equality and, empowerment of women including female education.
Innovative programs: Experience of Bangladesh, India and Thailand • Bangladesh Experience: Broad picture is high economic growth, infrastructure development, women’s agency (female secondary education) and NGOs presence for high human development. • Women’s agency in the form of women’s groups and female secondary education (targeted interventions like Female Secondary School Stipend Program) • The contribution of the NGO Gonoshayastha Kendra (GK) in raising health indicators in many areas is noteworthy. • Indian Experience: The regional experience shows that differences in health provisioning, improvements in child care, and health status of women explain malnutrition differences across states.
Indian Experience • The high performing states in India have shown: • rise in women’s nutrition status, • increase in the proportion of children under the age of three breastfed within one hour of birth, • rise in the percentage of children with diarrhoea who received ORS. • In India, Tamil Nadu and Kerala states have done well in reducing malnutrition. • The innovativeness and success of Tamil Nadu mid-day meal nutrition scheme is well known. • India : Public Distribution System (PDS) and nutrition programs • The Integrated Child Development Scheme (ICDS) launched in 1975, aims at the holistic development of
Indian Experience (contd.) • ICDS: children up to six years of age with a special focus on children up to two years, besides expectant and nursing mothers. • However, the progress has not been satisfactory. The Government wants to strengthen nutrition programs in India during 11th Five Year Plan. • There is a broad framework of action ‘children under six’ in the 11th Plan. • Three interventions involve integration of three related systems, focusing on: (a) food and nutrition;(b) health services; and (c)child care. • Many of these interventions can be taken care of through the ICDS. • ‘Universalization with Quality’ is the overarching goal of ICDS in 11th Plan.
Innovations • Thailand Experience: Thailand is considered as one of the most outstanding success stories of reducing child malnutrition in the post-1970s. • The success is attributable more to the direct nutritional programs by the govt. than only to rapid economic growth. • The country launched large focused programs on nutrition in 1977. The child malnutrition declined from 51% in 1979-82 to 17% in 1991. • These programs reduced child malnutrition through a mix of interventions including intensive growth monitoring and nutrition education on breastfeeding • and complementary feeding, strong supplementary feeding provision, iron and vitamin supplementation and salt iodisation along with primary health care.
Institutions, Rights Approach • Institutions and Service Delivery: Increase in public expenditure is important. India spends 0.9% of GDP on health. However, institutions to fit the needs and aspirations of 21stCentury are needed. • Social mobilization, community participation and decentralized approach are needed. • Rights Based Approach: Rights based approach is important. It may be difficult to make the right completely justiciable. • However, rights approach puts pressures on public action and would lead to effective implementation of the policies and programs (In India, Supreme Court intervention on nutrition programs).
conclusion • To conclude, improvement in incomes of poor, proper health services and quality environment are important for reduction in malnutrition. • Womens’ health and well being are crucial • However, in the short run, direct nutritional programs should be the priority. • Finally, political will is needed to sustain effective programs to reduce under nourishment and child malnutrition.