Download
1 / 30
340 likes | 496 Views
Launching at MMC - Aspergillus Galactomannan EIA - . “Galactomannan Screening for the Early Diagnosis of Invasive Aspergillosis” Dr. Vilma M. Co / Dr. Demetrio Valle Pledge of Support – Pfizer / Lifeline Message of Acceptance – Makati Medical Center Ceremonial MOA Signing

E N D
Launching at MMC - Aspergillus Galactomannan EIA - “Galactomannan Screening for the Early Diagnosis of Invasive Aspergillosis” Dr. Vilma M. Co / Dr. Demetrio Valle • Pledge of Support – Pfizer / Lifeline • Message of Acceptance – Makati Medical Center • Ceremonial MOA Signing ...........................Refreshments……………………….
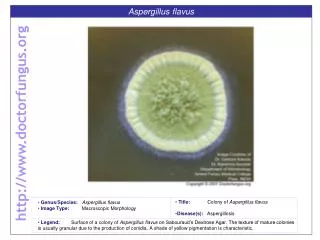
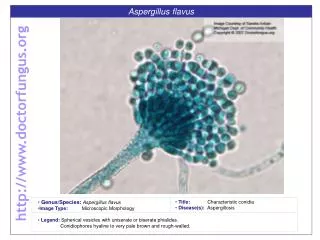
Aspergillus • fungus (or mold) that is common in the environment • soil • plants and in decaying plant matter • household dust • building materials • spices & some food items.
Different types of Aspergillus • Aspergillus fumigatus • Aspergillus flavus • Aspergillus terreus • Aspergillus nidulans • Aspergillus niger
Aspergillosis • allergic bronchopulmonary aspergillosis (also called ABPA) - a condition where the fungus causes allergic respiratory symptoms, such as wheezing and coughing, but does not actually invade and destroy tissue.
Aspergillosis • Invasive Aspergillosis - a disease that usually affects people with immune system problems. - the fungus invades and damages tissues in the body. - most commonly affects the lungs, but can also cause infection in many other organs & can spread throughout the body.
High-risk Patients • Invasive aspergillosis generally affects immunocompromised patients • bone marrow transplant or solid organ transplant, • people who are taking high doses of corticosteroids, • people getting chemotherapy for cancers such as leukemia. • persons with advanced HIV infection
Mode of Transmission • Inhalation of Aspergillus spores (i.e., in a very dusty environment) can lead to infection. • Studies have shown that invasive aspergillosis can occur during building renovation or construction. • Outbreaks of Aspergillus skin infections have been traced to contaminated biomedical devices.
Symptoms of Aspergillosis: • respiratory symptoms like wheezing, coughing and even fever • allergic sinusitis/bloody sputum • aspergilloma, or a “fungus ball” in the lung or other organs. • Lung aspergillomas usually occur in people with other forms of lung disease, like emphysema or a history of TB.
Invasive Aspergillosis • fever, chest pain, cough, and shortness of breath. • When invasive aspergillosis spreads outside of the lungs, it can affect almost any organ in the body, including the brain.
Incubation Period • Incubation time varies depending on host factors & exposure characteristics.
Diagnosis of Aspergillus infection • risk factors, symptoms, & P.E. findings • chest x-ray or CT scan of the lungs. • fungal culture of samples of respiratory secretions or affected tissues • biopsies of affected tissue • newer tests that can help monitor for invasive aspergillosis in high-risk persons who are severely immunocompromised
Aspergillus Galactomannan EIA CLINICAL UTILITY • used in conjunction with other diagnostic procedures to aid in the diagnosis of Invasive Aspergillosis. • microbiological culture • histological examination of biopsy specimens • radiographic evidence
Screening & Diagnosing IA in High-Risk Patients KEY BENEFITS : Screening high-risk patients with PlateliaTMAspergillus EIA, twice-weekly, provides early diagnosis of IA. Recent publications: • GM Ag was positive 6-10 days before onset of clinical signs • GM positivity preceded positivity of CT-Scan or culture by >1 week • PlateliaTMAspergillus EIA was most sensitive (compared to RT-PCR and -glucan) at predicting the diagnosis of IA in patients with hematologic disorder.
Screening and Diagnosing IA in High-Risk patients Comparison to Other Diagnostic Methods : J.Maertens JID 2002
Treatment of Invasive Aspergillosis • Voriconazole is currently first-line treatment for invasive aspergillosis. • itraconazole, lipid amphotericin formulations, caspofungin, micafungin, and posaconazole • Whenever possible, immunosuppressive medications should be discontinued or decreased.
Prevention • avoidance of dusty environments and activities where dust exposure is likely (such as construction zones) • wearing N95 masks in dusty environments • avoidance of activities such as gardening • air quality improvement measures such as HEPA filtration may be used in healthcare settings • prophylactic antifungal medication in some circumstances
ELISA SETUP WASHER INCUBATOR READER
PROCEDURE • immunoenzymatic sandwich microplate assay for the detection of Aspergillus galactomannan antigen • adult and pediatric serum samples • uses EBA-2 monoclonal antibodies which detect Aspergillus galactomannan.
Screening & Diagnosing IA in High-Risk patients • For maximum sensitivity, the test should be performedat least twice-weeklyduring hospitalization.For all positive patients, it is recommended that a newaliquot of the same sample be repeated as well ascollection of a new sample from the patient. • According to the EORTC/MSG criteria, two consecutivepositive results are required forclassification as truepositive.In daily practice, it is important that physicianssubmit a follow-up specimen upon receipt of the initialpositive result, ideally before initiating antifungal therapyto achieve the highest specificity using the test.
SPECIMEN TYPE & SPECIMEN HANDLING • Serum: • Collect 3 to 5 ml blood specimen in a serum separator tube (SST) without anti-coagulants. • Allow specimen to clot, then centrifuge specimen within 2 hours of draw to pellet cells below the gel. • Minimum volume of 1.0 ml serum following centrifugation is required. • Specimen should be stored at 2 to 8°C or frozen in a non-self-defrosting freezer & shipped with frozen gel packs or dry ice for overnight delivery
SPECIMEN TYPE & SPECIMEN HANDLING • BAL: • 1 to 3 ml collected in a sterile, screw-cap tube; • specimen should be stored at 2 to 8°C or frozen in a non-self-defrosting freezer • shipped with frozen gel packs or dry ice for overnight delivery
CAUSES FOR REJECTION of specimen • Lipemic, icteric, or hemolyzed specimens. • Specimens that have been stored at ambient temperature. • Specimens that have been stored at 2 to 8°C for >5 days. • If storage longer than 5 days is needed, samples should be frozen at -70°C.
ASSAY RANGE • The reference range is an index of <0.5. • Numerical index values will be reported. • Patients with an index of >0.5 are considered to be positive for galactomannan antigen. • Patients with an index of <0.5 are considered to be negative for galactomannan antigen.
ASSAY LIMITATIONS • A negative test result cannot rule out the diagnosis of Invasive Aspergillosis. • Patients at risk for Invasive Aspergillosis should be tested twice per week. • If a positive result is obtained, a second specimen should be collected and sent for testing immediately.
False-positive galactomannan test results • patients receiving piperacillin/tazobactam; interpret results in these patients with caution & confirm w/ other diagnostic methods. • Patients with intestinal mucositis caused by chemotherapy / irradiation, which allows for extra absorption of dietary galactomannan. • patients receiving Plasmalyte for IV hydration or if Plasmalyte is used for BAL collection.
TURNAROUND TIME • Same day (within 8 to12 hours of specimen receipt)