Download
1 / 33
330 likes | 453 Views
Cumulative Risk Male Female 1 in 9 1 in 8. Annual Burden of Cancer. 2005 806,300 912,000. With control of communicable diseases Increase in life expectancy Trends in smoking Changing life style. Cancer incidence and burden . ANTI-CANCER ACTIVITIES 1936

E N D
Cumulative Risk Male Female 1 in 9 1 in 8 Annual Burden of Cancer • 2005 • 806,300 912,000 With control of communicable diseases Increase in life expectancy Trends in smoking Changing life style Cancer incidence and burden
ANTI-CANCER ACTIVITIES 1936 First effort to set up a cancer hospital – appeal to King George V Memorial Fund by Dr.Muthulakshmi Reddy No Major national effort for 30 years after this Dr. Reddy also responsible for including cancer in the National Health Programme in the First 5-year Plan of Govt. Of India. 1965-71 Govt. of India committee Concept of Regional Cancer Centre 1982 Demographic registries 1985 NCCP
1949 Dr.Reddy had to justify the need for a Cancer Hospital Cancer perceived as a disease of the Aged a fatal / incurable disease Needed only Morphine to help their way to Eternity Perception of Cancer Then Cancer a major component of the National Health Plan Most states have a Cancer Centre Today’s Slogan Cancer is preventable, curable Stress on cancer survivors & Children of survivors Perception of Cancer now – 50 years later
National Cancer Registry Project (ICMR), 1981 & Other voluntary efforts • Setting up of 3 Demographic Registries • Bombay, Madras and Bangalore • A total of 14 Demographic Registries and 5 Hospital Cancer Registries (HCR) at present under NCRP • Only 3 are rural demographic registries • Six Demographic Registries outside NCRP network • ICMR Atlas Project – Data on cancer pattern in 82 districts from 105 centres in India. • Coverage: 6.9% of the population
Objectives of the National Cancer Control Programme, 1985 • Objectives based on the data from the Demographic registries • Primary prevention of Tobacco Related Cancers • Early detection and treatment of cancer of the cervix (extended to cover cancer at accessible sites cervix, breast and oral) • Enhancement of cancer treatment and control services through Regional Cancer Centres, Medical and Dental colleges. • Palliative care [added in – 1989]
Tobacco Research Activities in India • Chennai cohort study (300,000 men, aged ≥ 25 years) • 31% of total deaths due to any cancer was attributable to tobacco smoking ranging from 39% for stomach/oesophagus to 56% for lung/larynx cancers • Prevalence of tobacco smoking among men aged 35 and above is estimated to be 40% • Mumbai Cohort Study • 150,000 persons; Tobacco habit – 57.6% women; 69.3% men, smokeless tobacco use more common than smoking • Mortality rates higher for tobacco user than non-user • Global Youth Tobacco Survey (GYTS) among 13-15 yrs students • Prevalence ranged between 59% in Bihar, 4% in Goa; • 7% in Tamil Nadu and • Survey not carried out in Kerala.
MDCCP DATA FROM TAMIL NADU STATE (Women) Prevalence: Tobacco smoking: 3%; Tobacco chewing: 21% Age group Education Tobacco habit: with increasing age; with increasing education Frequency of women with awareness of Cancer as a term 79.2% Curability of cancer 45.0% Cancer Trt centres 32.4% Tobacco as a hazard 56.0%
Legislative Action • Anti-tobacco measures • Ban on tobacco advertisement • Ban on sale of tobacco near schools and colleges • Ban on smoking in public places • Ban on smoking in buses, airports. etc • Ban on sports promotion by tobacco companies • Hazards of tobacco in school books (hygiene, preventive medicine) • Monitoring of industries • Our recommendations • Preference to non-smokers as teachers in schools and colleges • Declare cancer a “Notifiable Disease”
CHINGLEPUT SURVEY OF CANCER 1961-63 Number surveyed : 10,775 Male : 3,239 Female : 4,842 Children : 2,092 Cancers detected : 67 Oral : 24 Cervix : 27 Breast : 16 Opportunistic Screening! % Stage Distribution of Carcinoma Cervix 1961 – 63 Foundation for the first ever pilot cancer control Programme – Kanchipuram 1967, WHO 1st INTERNATIONAL WHO CANCER CONTROL PROJECT KANCHIPURAM 1967
South Arcot District Level Cervical cancer early detection project: 1992-99 Objective To integrate the screening & education programme with the states’ permanent health infrastructure and delivery system This would significantly reduce cost Trained 258 Medical officers 672 VHNs 30 Block health educators 2 cytotechnicians Setup 2 Cytology laboratories in Cuddalore and Villupuram Total women examined 59314 Cancers detected 310 Early 12.3% Late 87.7% MOTIVATION POOR
Problems in the South Arcot Programme • VHN had multiple duties and received incentives for the FPP & immunization drive • No incentives in cancer detection programme • Fresh young women medical graduates – not confident • Compliance of women to be screened – Dependant on men folk!
Information, Education and Health Care Intervention IARC in collaboration with Nargis Dutt Memorial Cancer Hospital, Barshi Int. AreaNon Int. Area Ca Cervix 66% 25% Stage I & II
Major conclusions from various Indian studies • Population screening not practicable • For Cervical cancer VIA recommended at present • High priority and focus on • Educational Programmes • Serious effort to integrate screening with • routine health delivery system • Introduction of opportunistic screening can be considered
Technologic Advances • Enhanced Imaging • Enhancement in Tissue diagnosis • Molecular Diagnostics
Enhanced Imaging For evaluation of extent of disease / tumour size and tumour spread and monitor response to therapy Ultrasound CT Scan, Spiral CT MRI, PET Implications of sophisticated Imaging Expertise in interpretation Knowledge of relative merits of diff. available techniques Increase in cost of diagnosis
Molecular Markers • Molecular diagnostics • Prognostic & Predictive Markers • Minimal Residual Disease
Conceptual influences in Therapeutic Oncology • Preventive Oncology : Based on natural history of evolution of disease • Definition of early disease • Concept of Micrometastasis • Evaluation of extent of disease • Introduction of multi disciplinary approach
Multidisciplinary approach in Oncologic care • Appreciates limitation inherent in different modalities of treatment • Sequencing of different modalities • Surgery, radiation and chemotherapy based on biologic needs • Different in early disease and locally advanced disease
RESEARCH Synthesis of clinical practice studies & laboratory and research data Essential for progress Hereditary Cancer Clinic only one of its kind in India - 2002
Palliative Care: Palliative care medicine – a speciality A major component in cancer control Facilities in India Palliative care centres, hospices, hospital based centres Domiciliary services Andhra Pradesh 1 Tamil Nadu 5 Kerala 4 Assam 1 Uttar Pradesh 1 with 50 satellite Chandigarh 1 Rajasthan 1 centers Karnataka 4 Goa 1 55% of cancers Madhya Pradesh 2 have access to Maharashtra 3 Palliative Care New Delhi 2 Orissa 2 Calicut Centre WHO Demo Project PAIN CONTROL
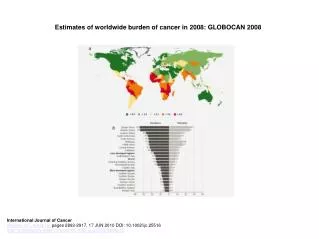
INCIDENCE AND BURDEN OF CANCER$ INDIA, 2001 & 2005 $ Estimates based on urban & rural registries Source: NCRP, ICMR Report (2004) & Individual Cancer Registry Reports
CIRs of Cervical & Breast cancers in India (Urban vs Rural registries) Trend of CIR of Cervical & Breast Cancers Urban India:1983-2002 Source: NCRP, ICMR Report (2005) & Individual Cancer Registry Reports
Trend in survival(%) at 5 years ALL: 0-25 Years : 1970-99 : (C.I)
Carcinoma Breast : Survival : HBCR All cases accepted for Treatment (All stages) Cancer Institute(WIA), Chennai * 9 year survival
Testicular Germ Cell Tumour Cancer Institute, Chennai • Treatment • Stage I : High Inguinal Orchidectomy - Observation • Stage II-III : High Inguinal Orchidectomy - CT • Role of Retroperitoneal lymphadenopathy is controversial
Disease profile in India Shift from communicable to Non communicable diseases
Health Budget and Cancer Budget (Government of India) % of Total outlay Health and Family Welfare 8.6% (Rs.6,283 crores) Health 2.0% (includes cancer Annual Rs.55 crores) Family Welfare 6.45% Indigenous medicine 0.18%
Change in cancer scenario : 1955-2005 • Improved Survival • Organ conservation • Concept of cancer prevention & • stress on early detection Result of advances in Technology & conceptual influences • High technology involves heavy financial investment • Increases cost and treatment • Reduces affordability
Future Directions • Identify individuals who have inherited or acquired defective suppressor gene • Identify precursor lesions & chemoprevention • Vaccine Based Strategies • Predictive Medicine – Pharmacogenomics • Array based methods for diagnosis, prognosis and choice of drugs for treatment