Download

1 / 6
0 likes | 7 Views
A dentist can improve denture fit with relines, adjustments, and implant-supported options for better chewing efficiency and comfort.

E N D
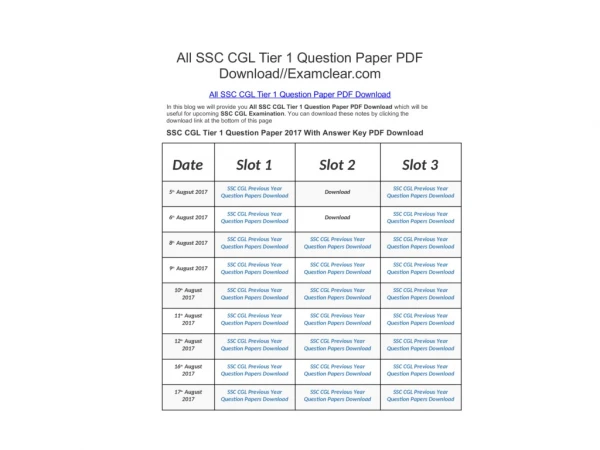
To a person staring down a throbbing molar on a cold January night in Worcester, the phrase root canal carries more heat than any clinical definition. I have treated patients who waited through Red Line delays, chewed on the other side for weeks, and swore they would rather give birth than sit in a dental chair again. Then they walked out saying, I should have done that sooner. The gap between fear and reality is wide here, so let’s close it. This guide brings together practical answers to the most common questions Massachusetts patients ask about root canals, how the process really feels, why an endodontist might be the right call, what costs and timing look like, and when to consider alternatives. Along the way, I will touch on where related specialties fit, from Dental Anesthesiology to Oral and Maxillofacial Radiology, since complex dental pain rarely belongs to one discipline alone. What a root canal actually is A root canal removes inflamed or infected pulp from inside a tooth, disinfects the canal system, and seals it so bacteria cannot sneak back in. Think of the tooth as a hard shell with a tiny network of tunnels at its core. When decay, cracks, or repeated dental work let bacteria reach those tunnels, the immune system fights a losing battle in a space too tight to swell safely. The result is severe pain, lingering sensitivity, and sometimes an abscess. Endodontics is the specialty devoted to diagnosing and treating disease of the dental pulp and the tissues around the root. Endodontists perform root canals all day, every day, and they invest in microscopes, micro-instruments, and 3D imaging that general practices may not have. A general dentist can and often does perform straightforward root canals. When the case is tricky - narrow, curved roots, retreatment, or a persistent infection - referral to an endodontist improves the odds and can shorten chair time. Do I really need a root canal? The answer starts with symptoms but ends with testing. Red flags include cold sensitivity that lingers more than 30 seconds, chewing pain, spontaneous throbbing, swelling, or a pimple-like bump on the gum near the tooth. Sometimes there is no pain at all, just a darkening tooth after trauma or an x‑ray finding. In the operatory, we confirm with a blend of science and judgment. Cold testing helps, but some teeth with dead pulp feel nothing and still harbor infection. Percussion and palpation tests check surrounding tissues. A periapical radiograph or, if needed, a cone-beam CT from Oral and Maxillofacial Radiology can reveal bone changes, missed canals, or hidden fractures. I have had patients swear it is the upper molar only to find the culprit is a lower molar referring pain upward, which is why we test neighboring teeth and do not chase pain alone. A root canal is indicated when the pulp is irreversibly inflamed or necrotic and you want to save the tooth. If the tooth is cracked below the gumline or lacks enough healthy structure to restore, extraction may be wiser. A thorough diagnostic workup, sometimes including evaluation by Oral Medicine if there are burning mouth symptoms or atypical neuralgia, prevents wrong-tooth treatment and avoids irreversible procedures on a tooth that might not benefit. How painful is it?
The procedure itself should not hurt. With modern local anesthetics and technique, most patients feel pressure and vibration but not sharp pain. Dental Anesthesiology plays a crucial role for anxious patients or those with medical complexity. Options range from buffered local anesthesia, to oral sedation, to nitrous oxide, to IV sedation monitored by an anesthesiologist. In Massachusetts, offices that provide sedation must meet strict training and permitting standards, and you should expect a pre-sedation evaluation if IV sedation is planned. What you feel afterward usually depends on the preoperative state of the tooth. Teeth that arrived hot - throbbing, swollen, difficult to anesthetize - often feel tender for 24 to 72 hours. Postoperative soreness typically responds to ibuprofen, acetaminophen, or a rotating schedule of both, unless your physician has told you to avoid them. If we needed to drain an abscess, or if your bite is high, tenderness can last a bit longer. Severe worsening pain, facial swelling, or fever after a root canal is uncommon and warrants a call the same day. I remember a Quincy firefighter who came in on his off day, jaw clenched, ready for the worst because his father’s root canal from the 80s was a horror story. Fifteen minutes after numbness, he was chuckling at the dental dam jokes. Technique and technology changed the experience. What happens during the appointment? The steps are routine but precise. After numbing, we isolate the tooth with a rubber dam so the field stays sterile. Under a dental operating microscope, we create a tiny opening, locate the canals, and work to the full length using electronic apex locators, files, and irrigants that dissolve tissue and kill bacteria where instruments cannot reach. We shape the canals gently to allow disinfection, then fill them with a biocompatible material and sealer. A temporary filling closes the access. For many first-time root canals on non-complicated teeth, the entire process takes 45 to 90 minutes. Retreatment or curved molars can take longer and may require two visits to let medication sit inside. If we suspect a vertical root fracture or an unusual anatomy, a quick CBCT scan guides decisions and prevents blind guesswork. Will I need a crown? If the tooth is a molar or premolar with a large cavity or existing restoration, yes, a crown is usually the safest way to prevent fracture. Front teeth with modest access openings sometimes do fine with a bonded composite restoration instead. I counsel patients to complete the final restoration within two to four weeks. Delays raise the risk of leakage or fracture. Once the root canal is finished, your general dentist or a Prosthodontics specialist designs the crown to handle your bite forces. If you grind at night or have a deep overbite, the restorative plan matters even more. Here is a simple, practical sequence Massachusetts patients find helpful: Complete the root canal and leave with a temporary filling and aftercare instructions. Return to your restorative dentist within 2 to 4 weeks for core build-up and crown preparation. Use a night guard if recommended to reduce fracture risk on the newly treated tooth. How successful are root canals? When properly diagnosed, cleaned, and sealed, success rates commonly land in the 85 to 97 percent range at five years, with many teeth healthy decades later. Success depends on factors we can control, such as cleaning, canal shaping, and coronal seal, and factors we cannot, such as unusual anatomy or microfractures. Endodontic retreatment or apical surgery can rescue a failing case, and both have solid track records when performed for the right reasons. One Boston-area case shows the value of persistence. A patient had a persistent lesion around a treated upper lateral incisor. Retreatment did not resolve it. A small apicoectomy performed in collaboration with Oral and Maxillofacial Surgery removed a missed lateral canal and sealed the apex retrograde. The lesion healed within six months. Matching the technique to the problem matters. How do antibiotics fit in? Antibiotics are not a substitute for treatment. They can help if there is spreading infection with fever or cellulitis, or if a patient needs to defer care for a day due to travel or illness, but their role is supportive. Dental Public Health principles guide antibiotic stewardship; unnecessary prescriptions drive resistance and gut side effects without helping the tooth. Once the canal is cleaned and sealed, antibiotics rarely add value.
What if I just extract the tooth? Extraction seems simpler upfront. For a fractured tooth, severe periodontal disease, or a tooth with a poor prognosis, it may be appropriate. The long view is different though. Replacing a molar typically means a dental implant or a bridge. Implants work beautifully in healthy bone, but they take time and money, and you need enough space and no active sinus issues. Bridges can be great, yet they require preparing neighboring teeth. Leaving a gap risks drifting, bite changes, and food impaction. For a roughly comparable molar with a reasonable crown-to-root ratio, saving the tooth with a root canal and crown often costs less than extraction plus implant in Massachusetts. There are exceptions. A tooth with a vertical root fracture or insufficient ferrule for a crown is a poor candidate for endodontics. Decisions improve when Endodontics and Periodontics collaborate to evaluate bone support and restorative feasibility. A brief consultation with Orthodontics and Dentofacial Orthopedics may even reveal a strategic plan to close a space orthodontically if extraction becomes the best path. How much does it cost in Massachusetts? Fees vary by provider and complexity. As a general range, a root canal on a front tooth might run 900 to 1,300 dollars, premolars 1,000 to 1,500, and molars 1,200 to 1,900 before insurance. A crown adds 1,200 to 2,000 depending on material and practice. Dental insurance often covers a percentage, typically 50 to 80 percent of endodontic fees, subject to annual maximums that commonly range from 1,000 to 2,000 dollars. If your plan resets on January 1, timing a crown in the next calendar year sometimes leverages benefits, but only if the tooth can safely wait. Waiting months is not wise on a vulnerable molar. Teaching clinics in Boston and Worcester occasionally offer reduced fees through dental schools or residency programs, where care is supervised by faculty. For eligible children, Pediatric Dentistry clinics coordinate care within MassHealth. If finances are tight, ask about staged care, such as completing essential endodontic steps now and final full-coverage restoration when feasible, while protecting the tooth with a durable interim buildup. Trade-offs exist, and your dentist can map them clearly. Why did the pain move or return after a few days? Postoperative flare-ups happen in a small minority of cases, especially teeth with severe preoperative pain, retreatments, or those with large lesions. The internal pressure shifts, residual bacteria release byproducts, or bite trauma inflames the ligament around the tooth. The tooth can feel high even if the filling is flat, because the ligament is swollen. Adjusting the bite, reinforcing anti-inflammatory medication, and, in rare cases, placing a short course of steroids or antibiotics resolve the episode. Leaving a contact number for after-hours support is part of good care, and patients appreciate it when the plan is laid out ahead of time. What if the tooth is cracked? Cracks complicate everything. An isolated craze line on enamel often needs no treatment. A crack that extends into the dentin can cause biting pain, especially on release. The classic test is biting on a tooth slooth and feeling a quick zing. If the crack reaches the pulp, a root canal can stop thermal sensitivity, yet the crack still threatens the root. Full cuspal coverage reduces risk of propagation. If a vertical root fracture is present, the prognosis is poor and extraction is usually recommended. Cone-beam imaging and transillumination under the microscope help distinguish salvageable cracks from hopeless ones. It takes honesty to say no to a root canal when the tooth will not endure long term. How do specialists work together on complex cases? Dentistry is a village. Endodontics addresses the canals. Prosthodontics plans the final restoration and occlusion. Periodontics ensures healthy gum and bone support and performs crown lengthening if a tooth needs more structure above the gumline. Oral and Maxillofacial Surgery steps in for apical surgery, complex extractions, or implant placement. Oral and Maxillofacial Radiology guides imaging decisions and interprets CBCT scans for nuanced anatomy or pathology at the root tips or sinus floor. Oral Medicine evaluates non-tooth pain sources like burning mouth, atypical odontalgia, or neuropathic pain. Orofacial Pain specialists assess temporomandibular disorders when jaw pain masks as tooth pain. Pediatric Dentistry adapts all of the above for developing teeth, where immature roots change strategy and regenerative endodontics might be considered. Orthodontics and Dentofacial Orthopedics influence long-term bite forces
that can protect or doom a restored tooth. Even Dental Public Health has a seat, shaping how prevention and access to care reduce the need for root canals in the first place. Integrated care does not mean more appointments for the sake of it. It means the right steps in the right order. A quick example: a patient with a deep carious lesion on a lower molar and minimal ferrule gets endodontic therapy first to eliminate infection. Periodontics performs crown lengthening to bring more tooth above the gum. Prosthodontics finalizes the crown design with occlusal harmony. The sequence saves the tooth that extraction alone would have sacrificed. How long will the numbness and tenderness last? Numbness from a mandibular block can last 3 to 6 hours; maxillary infiltration typically fades sooner, often within 2 to 3 hours. It Dentist Post Office Square Boston is common to feel dull tenderness when chewing for several days. Bruise- like sensitivity at the tooth’s ligament is normal. If you wear a night guard, use it. Avoid hard nuts and ice for a week. If pain worsens day by day rather than easing, call the office for a quick check. A simple bite adjustment sometimes makes a world of difference. Are there alternatives to a traditional root canal? Alternatives exist, but each comes with limits. Pulp capping or partial pulpotomy can preserve vitality in some young teeth with small exposures, especially in Pediatric Dentistry, but not when the pulp is necrotic. Regenerative endodontic procedures encourage continued root development in immature teeth with necrotic pulps. They serve a narrow but important group of patients. Extraction with implant or bridge replacement is a valid alternative when the tooth’s structure or prognosis is poor. https://www.mapquest.com/us/massachusetts/ellui-dental-695653641 There is ongoing research into biologic sealers, bioceramics, and minimally invasive shaping that preserve more dentin while maintaining disinfection. These refinements are changing technique details without changing the fundamental goal: eliminate infection and seal the system. How quickly should I act? If you have lingering pain to cold, spontaneous throbbing, or swelling, do not wait. Infections do not get better in a closed space. Massachusetts patients sometimes try to limp through a semester or a fiscal quarter, and we spend more time and money rescuing teeth that needed earlier help. Call your dentist or an endodontist within a day or two of strong symptoms. Most offices hold emergency slots, and true infections get triaged the same day. If you are asymptomatic but an x‑ray shows a dark halo at a root tip, the timeline is more flexible. We confirm vitality and monitor. If the tooth tests necrotic or the lesion enlarges, we plan treatment before bone loss accelerates.
What about pregnancy, medical conditions, and medications? Local anesthesia without epinephrine or with reduced epinephrine is safe in pregnancy, and we coordinate with your obstetrician. Second trimester is the most comfortable time for elective procedures. If you need urgent care at any point, we protect you and the baby with shielding for any necessary radiographs and adjust medication choices. For patients with cardiac conditions, joint replacements, or immunosuppression, we consult your physician and follow current guidelines on antibiotic prophylaxis. Anticoagulants are usually continued for root canal therapy; we manage minor bleeding locally. Diabetes slows healing, so we aim for good glycemic control around the appointment. If you are on bisphosphonates, that affects extraction risk more than endodontics, which is another reason to preserve the tooth when feasible. How do I choose a provider? Experience matters, and so does fit. Ask how often the provider performs molar root canals, whether they use a dental operating microscope, how they handle after-hours concerns, and how they coordinate with your restorative dentist. In Massachusetts, many endodontists publish success metrics and welcome case reviews. For anxious patients, ask about sedation options and the credentials of any Dental Anesthesiology team involved. For complex medical histories, look for practices accustomed to physician collaboration. I would rather see a well-executed root canal by a careful general dentist than a rushed one anywhere. The difference is not the sign on the door, it is the rigor of diagnosis, isolation, disinfection, and coronal seal, paired with honest boundaries about when to refer. What does aftercare look like? You will leave with instructions tailored to your case. Expect mild tenderness on chewing. Eat on the other side for a day. Brush and floss normally, avoiding snapping floss through a fragile temporary. If a temporary dislodges, call. If you feel high when you bite, return for an adjustment; do not try to tough it out. Schedule the crown promptly if recommended. Keep a simple pain log for a day or two if you are worried, noting what triggers the ache and how long it lingers. Patterns guide next steps. A brief reality check helps too. The goal is comfort and function, not perfection on day one. Healing on x‑ray can take months; your subjective relief arrives sooner. When pain is not from the tooth Not every ache is endodontic. Sinusitis can make upper molars feel tender to chew and sensitive to pressure changes on flights or in elevators. A night of clenching can mimic toothache. Trigeminal neuralgia or neuropathic pain presents as sharp, electric shocks that skip around rather than staying on one tooth. Oral Medicine and Orofacial Pain specialists are invaluable when the story does not fit, and we lean on them to avoid unnecessary root canals on healthy pulps. If your dentist hesitates before drilling, that pause is a sign of respect for your biology. Prevention still wins Root canals save teeth, but prevention saves time, money, and worry. Daily flossing or interdental brushes, fluoride toothpaste, and reducing frequent sugar exposures cut risk dramatically. Sealants in Pediatric Dentistry reduce molar decay. Orthodontics and Dentofacial Orthopedics can improve alignment that traps plaque. Periodontics promotes healthy gums that protect tooth roots. Dental Public Health reminds us that water fluoridation and access to routine care reduce the overall burden of endodontic disease across communities. Prevention may not make headlines, but it keeps you out of the chair when you would rather be hiking the Blue Hills or catching a game at Fenway. Final thoughts from the chair I have watched hundreds of Massachusetts patients reconcile their dread with the relief that follows a well-done root canal. They arrive braced and leave asking about lunch. The procedure is methodical, not mystical. When the diagnosis is sound and the plan respects the tooth’s structure, endodontic treatment is one of the most predictable ways we have to end dental pain and keep your own tooth working.
If you are unsure whether you need a root canal, start with an exam and a conversation. Ask the hard questions. Demand clarity on alternatives and costs. Good dentistry survives those questions easily. Ellui Dental 10 Post Office Square #655 Boston, MA 02109 https://www.elluidental.com 617-423-6777