Download
1 / 1
20 likes | 280 Views
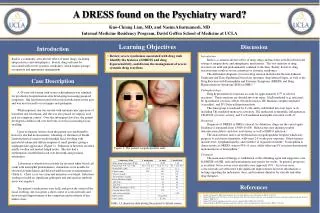
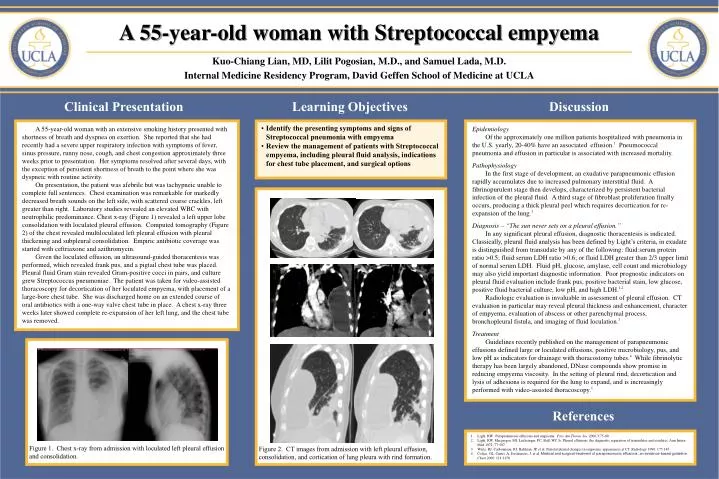
Figure 2. CT images from admission with left pleural effusion, consolidation, and cortication of lung pleura with rind formation. A 55-year-old woman with Streptococcal empyema Kuo-Chiang Lian, MD, Lilit Pogosian, M.D., and Samuel Lada, M.D.

E N D
Figure 2. CT images from admission with left pleural effusion, consolidation, and cortication of lung pleura with rind formation. A 55-year-old woman with Streptococcal empyema Kuo-Chiang Lian, MD, Lilit Pogosian, M.D., and Samuel Lada, M.D. Internal Medicine Residency Program, David Geffen School of Medicine at UCLA Clinical Presentation Learning Objectives Discussion A 55-year-old woman with an extensive smoking history presented with shortness of breath and dyspnea on exertion. She reported that she had recently had a severe upper respiratory infection with symptoms of fever, sinus pressure, runny nose, cough, and chest congestion approximately three weeks prior to presentation. Her symptoms resolved after several days, with the exception of persistent shortness of breath to the point where she was dyspneic with routine activity. On presentation, the patient was afebrile but was tachypneic unable to complete full sentences. Chest examination was remarkable for markedly decreased breath sounds on the left side, with scattered coarse crackles, left greater than right. Laboratory studies revealed an elevated WBC with neutrophilic predominance. Chest x-ray (Figure 1) revealed a left upper lobe consolidation with loculated pleural effusion. Computed tomography (Figure 2) of the chest revealed multiloculated left pleural effusion with pleural thickening and subpleural consolidation. Empiric antibiotic coverage was started with ceftriaxone and azithromycin. Given the loculated effusion, an ultrasound-guided thoracentesis was performed, which revealed frank pus, and a pigtail chest tube was placed. Pleural fluid Gram stain revealed Gram-positive cocci in pairs, and culture grew Streptococcus pneumoniae. The patient was taken for video-assisted thoracoscopy for decortication of her loculated empyema, with placement of a large-bore chest tube. She was discharged home on an extended course of oral antibiotics with a one-way valve chest tube in place. A chest x-ray three weeks later showed complete re-expansion of her left lung, and the chest tube was removed. • Identify the presenting symptoms and signs of Streptococcal pneumonia with empyema • Review the management of patients with Streptococcal empyema, including pleural fluid analysis, indications for chest tube placement, and surgical options Epidemiology Of the approximately one million patients hospitalized with pneumonia in the U.S. yearly, 20-40% have an associated effusion.1 Pneumococcal pneumonia and effusion in particular is associated with increased mortality. Pathophysiology In the first stage of development, an exudative parapneumonic effusion rapidly accumulates due to increased pulmonary interstitial fluid. A fibrinopurulent stage then develops, characterized by persistent bacterial infection of the pleural fluid. A third stage of fibroblast proliferation finally occurs, producing a thick pleural peel which requires decortication for re-expansion of the lung.1 Diagnosis – “The sun never sets on a pleural effusion.” In any significant pleural effusion, diagnostic thoracentesis is indicated. Classically, pleural fluid analysis has been defined by Light’s criteria, in exudate is distinguished from transudate by any of the following: fluid:serum protein ratio >0.5; fluid:serum LDH ratio >0.6; or fluid LDH greater than 2/3 upper limit of normal serum LDH. Fluid pH, glucose, amylase, cell count and microbiology may also yield important diagnostic information. Poor prognostic indicators on pleural fluid evaluation include frank pus, positive bacterial stain, low glucose, positive fluid bacterial culture, low pH, and high LDH.1,2 Radiologic evaluation is invaluable in assessment of pleural effusion. CT evaluation in particular may reveal pleural thickness and enhancement, character of empyema, evaluation of abscess or other parenchymal process, bronchopleural fistula, and imaging of fluid loculation.3 Treatment Guidelines recently published on the management of parapneumonic effusions defined large or loculated effusions, positive microbiology, pus, and low pH as indicators for drainage with thoracostomy tubes.4 While fibrinolytic therapy has been largely abandoned, DNase compounds show promise in reducing empyema viscosity. In the setting of pleural rind, decortication and lysis of adhesions is required for the lung to expand, and is increasingly performed with video-assisted thoracoscopy.1 Figure 1. Chest x-ray from admission with loculated left pleural effusion and consolidation. References • Light, RW. Parapenumonic effusions and empyema. Proc Am Thorac Soc 2006;3:75-80. • Light, RW, Macgregor, MI, Luchsinger, PC, Ball, WC Jr. Pleural effusions: the diagnostic separation of transudates and exudates. Ann Intern Med 1972; 77:507. • Waite, RJ, Carbonneau, RJ, Balikian, JP, et al. Parietal pleural changes in empyema: appearances at CT. Radiology 1990; 175:145. • Colice, GL, Curtis, A, Deslauriers, J, et al. Medical and surgical treatment of parapneumonic effusions: an evidence-based guideline. Chest 2000; 118:1158.