Download
1 / 35
350 likes | 489 Views
Malignant melanoma- risk factors (continued). Familial melanoma (10-15% of patients) Dysplastic nevi Large congenital nevi- about 6% develop MM. Clinical appearance. ABCD criteria: Asymmetry Border irregularity Color variation Diameter->6mm. Growth patterns. Radial growth:

E N D
Malignant melanoma- risk factors (continued) • Familial melanoma (10-15% of patients) • Dysplastic nevi • Large congenital nevi- about 6% develop MM
Clinical appearance • ABCD criteria: Asymmetry Border irregularity Color variation Diameter->6mm
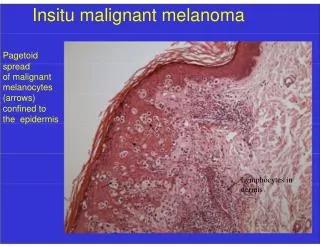
Growth patterns • Radial growth: • Tendency of melanoma to grow horizontally within the epidermis and superficial dermis, often for a prolonged time. • During this stage ,melonoma cells do not have capacity to metastasize • lentigo maligna, • superficial spreading and • acral/mucosal lentiginous
Vertical growth • The melanoma cells grows downwards into deeper dermal layers • This event is clinically marked by the development of a nodule in a relatively flat radial growth lesion • Develops capacity to metastasize
Clinicopathologic types of Malignant melanoma • Lentigo maligna: -Sun-exposed areas of elderly white patients, usually the face -Flat, slow-growing, prolonged in situ phase (ABCD criteria) -Proliferation of atypical melanocytes along the basal layer
Superficial spreading melanoma • The most common type of melanoma (70%) • Most commonly diagnosed in the fourth and fifth decades • Can occur in any location but more in intermittently exposed skin • Macroscopic-ABCD criteria apply • Nodule appearance- usually implies deep invasion • Microscopically- uniform atypical melanocytes, single and nesting
Acral lentiginous melanoma • Appears on the palms, soles and subungual areas • Diagnosed in older age groups • More common in black and oriental people • 10% of melanoma
Nodular melanoma • Represents about 15% of melanomas • Can affect all body surfaces, mainly the trunk, head and neck • Associated with short duration before diagnosis • ABCD criteria do not apply: can present as well-circumscribed smooth nodule in normal skin or in a nevus
Microscopy: • Cells are arranged in the form of poorly formed nests or nodules • The individual melanoma cells are • Large cells • Large irregular nuclei • Prominent red eosinophilic nucleoli
Laboratory methods • Melanin stains- Fontana-Masson • Immunohistochemistry- S-100 protein- HMB-45- more specific,
Spread and metastases • Epidermis to papillary dermis, reticular dermis and subcutaneous fat • Regional lymph node metastases are highly predictive of visceral metastases • Distant metastases- liver, lungs, gastrointestinal tract, bone, CNS
Staging • Tumor thickness (Breslow’s system)- most important prognostic factor. Measured from the top of the granular layer/ulcer base to the deepest tumor cell -Stage I:Less than 1mm- -Stage II:Between 1to 2mm- -Stage III:Between 2 to 4mm- -Stage IV:Over 4mm-
Prognostic factors (continued)-Level of invasion • Clark’s system: 5y survival level I- intraepidermal (in situ) 100% level II- in the papillary dermis 100% level III- filling the papillary dermis 88% level IV- in the reticular dermis 66% level V- in the subcutaneous fat 15% • Level of invasion has a significant impact on survival
Prognostic factors- continued • Ulceration- the second most important prognostic determinator of the primary tumor- bad prognosis • Mitotic activity- relationship between mitotic activity and prognosis: high mitotic rate associated with a bad prognosis