Download

1 / 10
100 likes | 225 Views
Qualified Clinical Data Registries. April 22, 2013 Quality Measures Workgroup. ATRA 2012 and Qualified Clinical Data Registries (QCDR). SATISFACTORY PARTICIPATION IN A QUALIFIED CLINICAL DATA REGISTRY.—

E N D
Qualified Clinical Data Registries April 22, 2013 Quality Measures Workgroup
ATRA 2012 and Qualified Clinical Data Registries (QCDR) SATISFACTORY PARTICIPATION IN A QUALIFIED CLINICAL DATA REGISTRY.— • “For 2014 and subsequent years, the Secretary shall treat an eligible professional as satisfactorily submitting data on quality measures under subparagraph (A) if, in lieu of reporting measures under subsection (k)(2)(C), the eligible professional is satisfactorily participating, as determined by the Secretary, in a qualified clinical data registry” • Secretary must recognize physicians that are “satisfactorily participating” in “qualified” clinical data registries for payment programs • Requires the Secretary to establish how to recognize a registry as qualified and suggests the following attributes: • ‘(I) has mechanisms for the transparency of data elements and specifications, risk models, and measures; • ‘‘(II) requires the submission of data from participants with respect to multiple payers; • ‘‘(III) provides timely performance reports to participants at the individual participant level; and • ‘‘(IV) supports quality improvement initiatives for participants.
CMS RFI on QCDR 2013 • Reporting entity requirements for qualified registry under the PQRS for 2014 and subsequent years or the EHR Incentive Program • What types of entities should be eligible to submit quality measures data on behalf of eligible professionals for PQRS and the EHR Incentive Program? Examples might include medical board registries, specialty society registries, regional quality collaboratives or other entities. • What qualification requirements should be applicable to such entities?
CMS RFI on QCDR 2013 • Measure Selection for PQRS and EHR Incentive Program • Should we require that a certain proportion of submitted measures have particular characteristics such as being NQF-endorsed or outcome-based? • Should QCDRs have apply to some entity for measure oversight? (HITPC described interest in measure quality) • Should measures be required to cover all 6 NQS domains? Or at least 3? • Participation Reporting Criteria • How many measures should an eligible professional be required to report on? • Should there be any requirement that the QCDR be able to report on both proprietary measures and eCQM from MU?
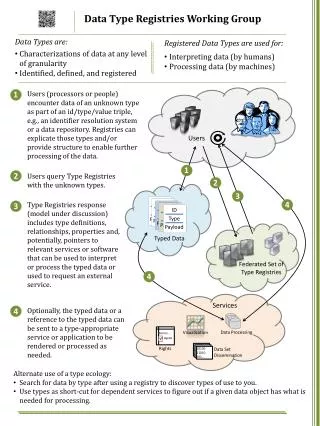
DITT Tasks Contribute recommendations on what additional attributes related to: 1. Privacy and Security 2. Data quality (completeness, timeliness, etc) 3. CEHRT Standards alignment (consume/produce CCDA or QRDA Level 3) 4. Business Rules (Do or Do Not Share Data, Do of Do Not Sale Data, etc)
Guiding Principles for QCDRS (from previous meeting) Define Registry Broadly Maximize Interoperability Manage Data Innovate on e-Measurement
Requirements for QCDR(from previous meeting) • Definition: Be an entity that may include but also may be independent from societies • Accept: Able to comply with standard for MU (e.g. 2014 SCC for eCQM CEHRT module) • Able to accept and incorporate PRO data into measures (e.g. at least one measure with a PRO data element) • EHR: able to automatically export and Registry able to accept CEHRT output • Analyze: Ensure data validity and integrity • Analyze/Export: Able to import/calculate/export QRDA cat 1&3 for 2014 eCQMs • Able to prove compliance and to pass data and process audit for privacy and security and data quality
Requirements for QCDR(provide reaction) • EHR must allow “automatic” export of relevant data to registries • Role: Accept Clinical Data • Registries must accept standardized EHR outputs (Consolidated CDA, QRDA cat 1&3) • Role: Data quality/Integration • Registries must ensure that data from EHRs are accurate, credible, and timely • Registries should be able to accommodate multisource data Accept: Able to accept multisource ( human abstracted, claims, clinical, administrative) data • Role: Design Quality Measures and Perform Analytics • Measure quality: How can we be sure that measures are of high quality? Should they be NQF endorsed? • Measures Interoperability: e-Measures must use value set and logic that are consistent with HHS standards • Ability to import/calculate/export should require Certification • Role: Reporting data and results • Measure/Data Interoperability: Submit data to CMS (?and commercial payers) via QRDA or the appropriate SCC Standard • Publically reports all measures, numerator, denominator, exclusions and rationale • ? Should provider be afforded opportunity to review all reports prior to publication?
Additional Questions What other roles will be required for CEHRT? What other roles are required for QCDR? What level of verification is appropriate for each? Attestation, Certification, Auditing?
Framework Payers Intermediaries Clinical Data Sources