Download
1 / 17
170 likes | 332 Views
Diuretics drugs that increase sodium and water excretion from the body by an action on the kidney. (2006). According to Katzung's Basic & Clinical Pharmacology . McGraw-Hill Medical; 9 edition (December 15, 2003). Proximal convoluted tubule

E N D
Diuretics drugs that increase sodium and water excretion from the body by an action on the kidney. (2006)
According to Katzung's Basic & Clinical Pharmacology. McGraw-Hill Medical; 9 edition (December 15, 2003)
Proximal convoluted tubule • - isosmotic reabsorbtion of aminoacids, glucose and cations • - secretion and reabsorption of weak acids – org. anions • sodium and water reabsorption – 50 % of sodium reabsorption • free water permeation • - bicarbonate reabsorption – HCO3-is not reabsorbet itself carbonic anhydrase According to Katzung's Basic & Clinical Pharmacology. McGraw-Hill Medical; 9 edition (December 15, 2003)
Thick portion of the ascending limb of the loop of Henle • - pumps Na+, K+ and Cl- into interstitium - 30-40 % of Na+ • major site of Ca2+ and Mg+ reabsorption – driven by K+ According to Katzung's Basic & Clinical Pharmacology. McGraw-Hill Medical; 9 edition (December 15, 2003)
Distal convoluted tubule pumps Na+ and K+ out of lumen – 10 % of Na+ Ca2+ reabsorption – parathyroid hormone – Na+/Ca2+ exchanger According to Katzung's Basic & Clinical Pharmacology. McGraw-Hill Medical; 9 edition (December 15, 2003)
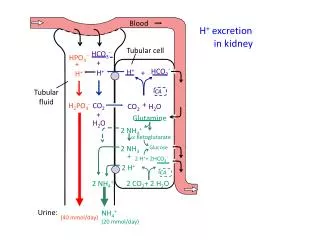
Cortical collecting tubule Na+ reabsorption/ K+ secretion – aldosteron a) expression of Na+ channels at apical membrane, b) increase expression and activity of Na+/K+ATP-ase exchange – 2-4 % Na+ reabsorbed H+/K+ATPase - primary site of urine acidification – movement of K+ is accompanied by an equivalent movement of H+ According to Katzung's Basic & Clinical Pharmacology. McGraw-Hill Medical; 9 edition (December 15, 2003)
Carbonic anhydrase inhibitors • Loop diuretics • Thiazide diuretics • Potasium-sparing diuretics • Osmotic diuretics
1. CARBONIC ANHYDRASE INHIBITORS Acetazolamide, dorzolamide inhibition of CA in brush border and intracelular CA in PCT – depletion of bicarbonate – metabolic acidosis HCO3- Na+ inside the tubuli exchange for K+ in DCT – mild hypokalemia after 2-3 days HCO3- excretion slows (HCO3- depletion) – diuretic action is self limiting CA in ciliary epitelium – secretion of HCO3- into aqueous humor – intraocular pressure - glaucoma CA in choroid plexus – secretion of HCO3- into cerebrospinal fluid – acidification – hyperventilation – protect against mountain (high-altitude) sickness
1. CARBONIC ANHYDRASE INHIBITORS Clinical uses glaucoma mountain (high-altitude) sickness significant metabolic alkalosis Toxicitydrowsiness and paresthesias alergic reactions (sulfonamides) renal stones – precipitation of Ca2+ salts in alkaline urine potassium wasting
2. LOOP DIURETICS Furosemide - act from luminal site - inhibits the cotransport Na+ K+ 2Cl-Na+ excretion from 1 % to 35 % - massive sodium chloride diuresis - reabsorption of Ca2+ and Mg2+ - pulmonary vasodilating effect + venodilatation - - i.v. or orally - short acting – 3-6 h Clinical use heart failure refractory oedema renal failure with fluid overload hypertension hypercalcaemia
2. LOOP DIURETICS Pharmacokinetics F + rapid, protein binding > 95 %, elimination mainly via kidney (filtration and secretion), t1/2 = 2 h prolonged in renal failure 10 hAdverse effects acute renal failure – prerenal failure - 2,5 l/h hypokalaemia (! digoxin !) metabolic alkalosis hypomagnesaemia – correct K+ (! digoxin !) hyperuricaemia ototoxicity alergic – rare blood dyscrasias Li+
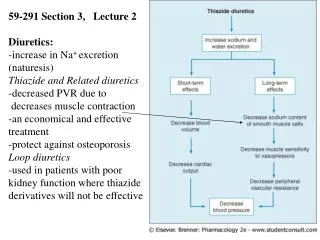
3. THIAZIDE DIURETICS • Hydrochlorothiazide • act from luminal site- inhibit Na+ Cl- cotransportin early segment of DCT - Na+/Ca2+-ATPase - Ca2+ reabsorption- mild inhibition of CA- orally in the morning – onset 2 h - duration 6-12-20 h (dependent on drug)Clinical use hypertension cardiac failure resistant oedema prevention of stones – idiopatic hypercalciuria + maintain high urine output diabetes insipidus
3. THIAZIDE DIURETICS Pharmacokinetics orally – F = 60-80 %, protein binding 65%, Vd = 0,5-1,1 l/kg, elimination – kidney 95% unchanged - CLtot of hydrochlorothiazide = CLCR main mech. is GF but also secretion is involved (interaction at OAT), t1/2 = 6-8 h.Adverse effects impotence hypokalaemia and hypomagnesaemia (! digoxin !) hyponatremia hyperuricaemia impaired glucose tolerance allergy Li+
4. POTASIUM-SPARING DIURETICS inhibit Na+/K+ exchange in CCL – K+ retention + mild natriuresis combination with thiazides and loop diuretics Spironolactone act from basolateral site in CCL– competitive antagonist on intracelular aldosteron receptor expression of Na+ channels and Na+/K+ ATPase Clinical useprimary hyperaldosteronismsecondary hyperaldosteronism – cirhosis, heart failure Adverse effectsmen - gynaecomastia, breast tenderness, women – menstrual irregularity – oestrogen action tumours in rodent
4. POTASIUM-SPARING DIURETICS • Amiloride, triamteren • - act from luminal site (apical, canalicular) in CCL – block Na+ channels Na+ clearance and K+ and H+ clearance • long acting 12-24 h (8 h by Ritter 2000)Clinical use potassium wasting – diuretics – combination • Adverse effects !!! hyperkalemia !!! – monitoring – risk factors diabetes mellitus, ACEI, NSAID metabolic acidosis • Pk triamteren – t1/2 = 2 h, diuresis 8 h, metabolized prior to excretion
5. OSMOTIC DIURETICS • Manitol, ureal, glycerine • filtered at the glomerulus but poorly reabsorbed - „holds“ water in the lumen by virtue of its osmotic effect - proximal tubulus - descending limb of the loop of Henle - collecting tubule volume of urine + Na+ lost • - volume of plasma (water from the tissues to the circulation) – unsuitable for treatment of oedema (!!! cardiac failure !!!)
Clinical use to maintain high urine flow - solute overload from severe hemolysis or rhabdomyolysis reducing intraocular pressure in acute glaucoma reducing intracranial pressure Adverse effect pulmonary edema headache, nausea, and vomiting