Spinal Cord Injuries
540 likes | 920 Views
Spinal Cord Injuries. Bradley J. Phillips, MD Burn-Trauma-ICU Adults & Pediatrics. Incidence. 8,000-10,000 per year Mechanisms MVC 48% Falls 21% Assaults 15% Sport-related 14% (majority diving). Incidence. 50% involve cervical spine (C5-6) 40% lead to quadriplegia Co-morbidity

Spinal Cord Injuries
E N D
Presentation Transcript
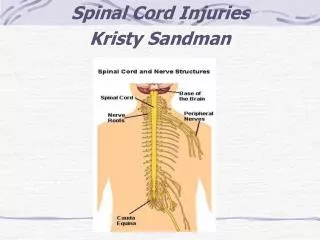
Spinal Cord Injuries Bradley J. Phillips, MD Burn-Trauma-ICU Adults & Pediatrics
Incidence • 8,000-10,000 per year • Mechanisms • MVC 48% • Falls 21% • Assaults 15% • Sport-related 14% (majority diving)
Incidence • 50% involve cervical spine (C5-6) • 40% lead to quadriplegia • Co-morbidity • Limb fractures - 67% • Intrathoracic - 53% • Head injury - 33%
C5 C6 Cervical Spine Fractures
Anatomy & Biomechanics • Spine stability dependents • bone • ligaments • joints • applied force • axial • extension • rotation
Biomechanics • Upper cervical spine • C1 - vulnerable to axial load (Jefferson’s fx) • C2 - vulnerable to hyperextension (Hangman’s fx) • Lower cervical spine • C5-C7 - most common fx and dislocation • highly mobile • vulnerable to hyperextension • significant neurologic injury
Biomechanics • Rotation + Flexion • unilateral locked facet • severe - bilateral locked facet • usually stable and no sig ligamentous disruption or neurologic injury • Thoracic spine • direct blows or extreme hyperflexion • axial loading - compression or burst fx • T12- L1 vulnerable to hyperflexion/axial force • severe ligamentous injury, retropulsion of fragments
Pathophysiology • Actual mechanical transection rare • Neural action potentials will not cross • Immediate vascular disruption • Leads to necrosis • Rapid swelling of cord tissue • Histologic changes max at 72 hours • May extend for two segments proximally and distally !!!
Diagnosis • History • mechanism • associated injuries • head and spine injury 6-15% of patients • Physical exam • MUST BE • conscious and alert • non-intoxicated • no distracting injury
Risk Factors for Cervical Injury • Blunt • potentially any blunt mechanism of injury • Penetrating • low risk
Diagnosis • Physical • palpate entire spine • thorough neuro exam including • sensory (pinpoint, position) • sacral function (rectal,bulbocavernosus reflex) • Complete or incomplete • Clinical level is lowest nerve root providing good sensation/motor function
C4-sensation to nipple motor to trapezius C5-sensory lat arm motor deltoid/biceps C6-sensory thumb/index motor wrist extension C7-sensory ring finger motor wrist flex/triceps C8- sensory little finger motor finger flexors T1-sensory medial arm motor hand intrinsic L1 - sensory pubis/lower abdomen L2 - sensory ant thigh motor flexion at hip L3 - sensory knee and motor knee extension L4 - sensory medical calf motor dorsiflex ankle L5 - sensory lat calf and motor dorsiflex toes S1 - sensory fifth toe/heel motor plantar flex toes S2/3 -sensory back thigh/buttock motor anal spinchter contraction S4 - sensory perineum S5 - sensory perianal Markers of Nerve Root Function
Pitfall Unwise to predict neurologic outcome within 48 hours of apparently complete spinal cord injury
Xrays needed? • Cervical • neck tenderness, intoxication, abnormal neuro exam, distracting injury, difficult clinical exam • Thoracolumbar • spine tenderness, MVC ejections, MCC, falls > 10 ft, neurologic deficit, difficult clinical exam
Radiology Exam • Radiography bony deformation full bony excursion and damage at time of injury • Films • Cervical spine • lateral • odontoid • AP • Flexion/extension • ? obliques
Lateral View • Adequate film C1-T1 top • Column alignments • Anterior line of vertebral body • Posterior line of vertebral body • Junction of laminae with spinous process • Tips of spinous process • Curvature overall
Lateral View - Helpful Measurements 1. prevertebral space < 5 mm 2. atlantodental interval 2.5-3 mm 3. sup-inf vertebral align < 2.7 mm 4. ant-post body height < 3 mm 5. spinal canal width > 13 mm 2. 1. 3. 4. 5.
Cervical Views Obliques Odontoid AP
Pitfalls Absence of typical signs of spinal fracture on plain radiograph does not guarantee the absence of a fracture or predict stability
CT better than plain Xray? • Superior for Occiput - C3 in altered mental status patients(Schenarts, J Trauma, 2001) • recommend obtain at time of CT Head • Helical CT + plain films increased accuracy of detecting cervical spine injury from 54% to 100%(Barba, J Trauma, 2001) • recommend full Cervical CT at time of CT Head • Conclusion: CT with plain films better in altered mental status and should be obtained with CT Head
Spine Instability • Indicators of instability on plain radiographs • > 5 mm subluxation • bilateral jumped facets • burst fractures with bone fragments in canal • widening of interspinous space • fractures of posterior element • Columns - 2 of 3 damaged • Flexion/extension • plain radiographs - no pain & active full motion
Cervical Spine Clearance Intubated and Difficult Exam No Yes Yes Yes Consult Spine Spine CT/MRI Meets Clinical Criteria (A) Abnormal Plain Films Clear Clinically No No Yes Clinical exam within 72 hours Consult Spine Spine CT/MRI Abnormal Plain Films No Yes No Yes Yes Abnormal Neurologic Exam Consult Spine Fluoroscopic Flex/Ex Consult Spine: MRI OR within 72 hours No No Yes Yes Posterior Cervical Midline Tenderness Hard Collar F/U Spine Service Meets High-Risk Criteria (B) Consult Spine: MRI No No D/C Collar after Period of Observation Consult Spine Spiral CT Occiput-C3 Criteria B High speed MVC (>35mph) MVC with death at scene Fall > 10 feet Significant closed head injury Referred cervical neurologic signs/symptoms Pelvic or multiple extremity fractures Criteria A No midline tenderness No focal neurologic deficit Normal alertness Negative toxicology screen No painful, distracting injury
Treatment • Immobilization • Drug Therapies • Steroids • GM-1 Gangliosides • Surgical management • Rehabilitation
Steroids: blunt trauma • “Standard of Care” • National Acute Spinal Cord Study • within 8 hours of injury • methylprednisolone 30mg/kg load, 5.4 mg/hr x23 hrs. • result: slight but significant improvement in motor function and sensation at 6 months • NASCS 2nd trial • some benefit of 48hrs of steroids, but significant morbidity (severe sepsis and pneumonia)
Surgical Management • Subluxation/angulation • immobilization with traction • not recommended with fractures • Braces • Halo brace • Minerva jacket/vest
Surgical Management • C1 rotatory subluxation- after reduction treatment with Halo 3 months • C1 fx (Jefferson) - usually stable treat with hard collar (ligament injury- Halo) • Odontoid fx - depend on type • Type I and III usually hard collar/halo 3 mos • Type II - young (halo) and older (ORIF) • C2 fx (Hangman’s) - Halo at least 3 months
Surgical Management • Lower cervical • fracture/dislocation - posterior ORIF with/without collar • compression/burst - anterior ORIF or halo • Thoracolumbar • compression without subluxation usually stable require brace only • severe subluxation/retropulsion bone fragments require ORI
Early - Pro provide better restoration of bone alignment earlier decompression may improve neural function early stabilization prevents secondary cord injury early mobilization prevent pulm complications Early - Con adequate alignment by traction and closed manipulation early removal of bone fragments does not improve outcome benefits of early mobilization obtained by active PT Injury made worse Timing of Surgery
Timing of Surgery • Axiom - indications for early surgery • progressively worsening deficit • persistent CSF leak • failure to achieve spinal alignment by closed methods
Complications • *Cardiovascular • hemodynamics • sinus bradycardia • *Venous Thromboembolism • *Pulmonary problems • Skin breakdown (most avoidable) • Autonomic Hyperreflexia (usually above T6) • Muscle spasiticity (trial of baclofen)
Complications • Gastrointestional • ileus (acutely need gastric decompression!!!) • peritonitis • Malnutrition • Hyperkalemia crisis (avoid succinylcholine) • GU complications (infections) • Heterotopic ossification
Cardiovascular Instability • Injury above T1-T2 • disruption of descending sympathetic fibers • Effects = “neurogenic shock” (not spinal shock) • vasodilation • myocardial dysfunction • bradycardia
Cardiovascular Instability • Treatment • aggressive fluid resuscitation • rule-out injury with continued blood loss • vasopressors - alpha-agonists
Venous Thrombosis • Major risk factor • ? Eventually all develop DVTs • Significant PE in 10% • Therapy • Mobilization/leg elevation • Heparin (LMW vs Standard) • Caval filters
Pulmonary Complications • Leading cause of death • pneumonia/atelectasis • as high as 40% in quadriplegia (older study) • Avoid intubation if possible • aggressive pulmonary toilet (suctioning, quad cough, avoid NGT/FT if possible) • positioning changes (manual, ROTO bed) • check spontaneous TV frequently • “Ondine’s curse” - ok awake, but lose respiratory drive asleep
Rehabilitation • Begins immediately • Objectives • maintain full range of motion of joints • use of orthotics to prevent contractures • muscle strenghtening • patient education • self-range techniques • activities of daily living