Download
1 / 28
280 likes | 792 Views
Healthcare Associated Pneumonia. Barbara G. Bielska, M.D. Clarian Arnett Health Infectious Diseases Department. Definitions. HCAP-signs, symptoms and radiographic presence of PNA in CAP patients with recent contact with the healthcare system HAP- 48-72 hrs after hospital admission

E N D
Healthcare Associated Pneumonia Barbara G. Bielska, M.D. Clarian Arnett Health Infectious Diseases Department
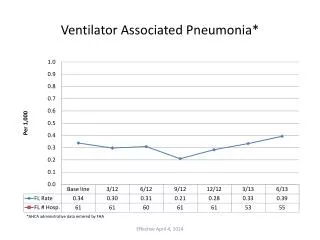
Definitions • HCAP-signs, symptoms and radiographic presence of PNA in CAP patients with recent contact with the healthcare system • HAP- 48-72 hrs after hospital admission • VAP- 48-72 hrs after endotracheal intubation
Epidemiology of Pneumonia • Leading cause of infectious diseases related death globally and in the US • CDC (2006) more than 56 K deaths • 1.2 mln out of 35 mln annual US hospitalizations • US expenditures > $8 billion annually • 300K cases of HAP/y with associated mortality rate 30-70% • HAP lengthens hospital stay by 7-9 days
Healthcare Associated PneumoniaATS/IDSA Guidelines 2005 • Hospitalization for 2 days or more in the preceding 90 days • Residence in the NH or ECF • Home infusion therapy ( including abx) • Chronic dialysis within 30 days • Home wound care • Family member with a MDR pathogen
HCAP as clinical entity • Large, heterogeneous patient population with a poorly defined conglomeration of risk factors that may increase the risk of infection with a drug resistant pathogen
HCAP Definitionsby Study • Kollef at al 2005 ( hospitalization in 30 d, transfer from other facility, chronic HD) • Carratala at al 2007 (hospitalization in 90 d, NH /ECF residence, home infusions/IV therapy, attended hospital/HD clinic past 30 d, IV chemotherapy past 30 d) • Shorr at al 2008 (hospitalization in past 90 d, NH/ECF, chronic dialysis, immunocompromised state)
HACP Definitions by Study • Venditti at al 2009 ( hospitalization/surgery in the past 180 d, NH/ECF, attended hospital/HD clinic in the past 30 d, IV chemotherapy in the past 30 d) • Shindo at al 2009 ( hospitalization in past 90 d, NH/ECF, home infusions/ IV therapy, chronic dialysis, home wound care,
The Magnitude of the HCAP PopulationCAP vs. HCAP by study • Kollef ’05- CAP-69.2%, HCAP-30.8% • Micek ‘’07 and Shorr’ 08- CAP-32.6%, HCAP- 67.4% • Carratala ’07- CAP-82.7%, HCAP- 17.3% • Venditti’ 09- CAP- 71.2%, HCAP-28.8% • Shindo ’09- CAP- 62%, HCAP- 38% • Avarage CAP-63.9%, HCAP- 36.5% • % HCAP of community dwelling adults hospitalized for pneumonia
Etiology and Outcomes HCAP vs. CAP • Micek at al ’07single center retrospective cohort analysis ( US) 2003-05 • HCAP (n- 431), CAP (n-208) • S.aureus (% MRSA) 44.5% (68.8), 25.5% (47.1) • S.pneumoniae 10.4%, 40.9% • P.aeruginosa 25.5% , 4.8% • H. influenzae 4.2%, 17.3% • Legionella sp.0.2%, 3.4% • HLS not provided, In hospital mortality 24.6% VS. 9.1%
Etiology and Outcomes HCAP vs. CAP • Venditti at al ’09 multicenter prospective observational study ( Italy, 55 hosp. ’07) • HCAP (n-90), CAP (n-49) • Variable no pathogen data • HLS in days, mean 18.7 vs. 14.7 , p-value<0.05 • In hospital mortality 17.8% vs. 6.7%, p-value <0.05
Etiology and Outcomes HCAP vs. CAP • Shindo at al ’09 single center retrospective observational study (Japan), 2005-07 • HCAP (n-141), CAP (n-230) • Pathogen (%, culture positive) • S. pneumoniae -13.5, 19.1 • S.aureus (% MRSA)- 9.9 (35.7), 6.1 (14.3) • Pseudomonas sp.-5.7, 1.7 • No pathogen identified- 45.4, 52.6 • Previous abx past 90 d (%)-63.1, 20.9 • In hospital mortality %- 21.3, 7.4
HCAP or Drug Resistant PNA • Variables independently associated with resistant pathogen : MRSA, P.aeruginosa, ESBL Klebsiella sp /other non fermenting GNR’s, • Recent hospitalization, 3 mo • Nursing Home residence/ LTCF, poor functional state • Long term hemodialysis • ICU admission • Broad spectrum antibiotics use, 3 mo
Patient’s Risk for Resistant Pathogen • Knowledge of reason for prior admission • Duration of prior hospitalization • Receipt of antibiotic therapy • Known MDR pathogen circulating in community or hospital • Immunosuppressive disease present or therapy given • Search for drug resistant pathogen specific risk factor is complicated by study’s statistical power, selection bias, limitations of case control study design • Limited evidence for community dwellers
HCAP, HAP, VAPDiagnosis • Difficult, no reliable tools to determine if patient has PNA • No reliable methods to determine causative pathogen when PNA present Sampling methods for ventilator-associated pneumonia: Validation using different histologic and microbiological references. Crit Care Med. 28: 2000; 2799-2804. New infiltrate on CXR, fever, purulent sputum other signs of clinical deterioration Clinical method was shown to be specific for HAP in only 27 of 84 patients in a series reported by Fagon at al. Evaluation of clinical judgment in the identification and treatment of nosocomial pneumonia in ventilated patients. Chest. 103: 1993; 547-553
Conditions mimicking PNAin critically ill • Congestive heart failure • Pulmonary embolism • Atelectasis • Acute respiratory distress syndrome (ARDS) • Pulmonary hemorrhage • Drug reactions
Imperfect diagnostic tests • Blood cultures, limited role, sensitivity is only 8% to 20% • Sputum neither sensitive, nor specific • Tracheo-bronchial aspirates- high sensitivity, weakness- does not differentiate between pathogen and colonizer • Hospital-acquired pneumonia: Risk factors, microbiology, and treatment. Chest. 119: 2001; 373S-384S. BAL, PSB’s do not differ from less invasive tests in terms of sensitivity, specificity or, more importantly, morbidity and mortality luckof consensus on the role of invasive diagnostic testing for HAP, subject of ongoing debate • Noninvasive versus invasive microbial investigation in ventilator-associated pneumonia: Evaluation of outcome. Am J Respir Crit Care Med. 162: 2000; 119-125. • Invasive and noninvasive strategies for management of suspected ventilator-associated pneumonia: A randomized trial. Ann Intern Med. 132: 2000; 621-630.
HCAP, HAP, VAPTreatment • Delay in empiric antibiotics use, worse outcomeInternational conference for the development of consensus on the diagnosis and treatment of ventilator-associated pneumonia. Chest. 120: 2001; 955-970. • Mortality with prompt abx use 30% vs. 91 % when delayedNosocomial pneumonia: A multivariate analysis of risk and prognosis. Chest. 93: 1988; 318-324 • Regimens in patients with no known risk factors for MDR pathogens, and who have early-onset pneumonia (within 5 days of hospitalization) should include coverage forEnterobacter spp., E. coli, Klebsiella spp., Proteus spp., and Serratia marcescens), Haemophilus influenzae and Streptococcus pneumoniae, MSS. aureus
HCAP, HAP, VAPTreatment • ceftriaxone or a quinolone (e.g., ciprofloxacin or levofloxacin) or ampicillin-sulbactam or eratpenem • fluoroquinolone in the empirical regimen of patients with penicillin allergies • penicillin skin testing – a mean to decrease fluoroquinolones use • A pilot study of penicillin skin testing in patients with a history of penicillin allergy admitted to a medical ICU. Chest. 118: 2000; 1106-1108.
Antibiotics for Empirical Therapy of Hospital-Acquired Pneumonia * in Patients at Risk for Multidrug-Resistant Pathogens • Antibiotic Adult Dosage † • Antipseudomonal cephalosporin • Cefepime 1-2 g every 8-12 hr • Ceftazidime 2 g every 8 hr • Carbepenems • Imipenem 500 mg every 6 hr or 1 g every 8 hr • Meropenem 1 g every 8 hr • Beta-lactam–beta-lactamase inhibitor • Piperacillin-tazobactam 4.5 g every 6 hr • Aminoglycosides • Gentamicin 7 mg/kg/day • Tobramycin 7 mg/kg/day • Amikacin 20 mg/kg/day • Antipseudomonal quinolones • Levofloxacin 750 mg/day • Ciprofloxacin 400 mg every 8 hr • Vancomycin 15 mg/kg every 12 hr • Linezolid 600 mg every 12 hr • Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med 2005;171:388-416.
Duration of treatment • No consensus, initial low suspicion, no change in clinical status- dc in 72 hrs Short-course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription. Am J Respir Crit Care Med. 162: 2000; 505-511. • Guided by severity, time to clinical response, and the pathogenic organism • Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare associated-pneumonia. Am J Respir Crit Care Med. 171: 2005; 388-416. • Treat for at least 72 hours after a clinical response is achieved • International conference for the development of consensus on the diagnosis and treatment of ventilator-associated pneumonia. Chest. 120: 2001; 955-970.
Recommendations for Assessing Response to Treatment • Modifications of empirical therapy should be based on results of microbiology testing in conjunction with clinical parameters. • Clinical improvement of HCAP usually takes 2 to 3 days and therefore therapy should not be changed during this period unless there is a rapid clinical decline. • Narrowing therapy to the most focused regimen possible on the basis of culture data (de-escalation of antimicrobials) should be considered for the responding patient. • The nonresponding patient should be evaluated for possible MDR pathogens, extrapulmonary sites of infection, complications of pneumonia and its therapy, and mimics of pneumonia. • Testing should be directed to whichever of these causes is likely after physical examination of the patient.
Prevention Measures • Based on expert opinion rather than hard data • CDC published a set of 74 recommendations for preventing NAP , only 15 strongly supported by well-designed experimental or epidemiologic studies • 14 out of those 15 dealt with surveillance, education, hand washing, sterilization, proper use of gloves, value of vaccination, and sanitation • Prophylactic antibiotics not be used routinely , only one supported by well-designed studies • Centers for Disease Control and Prevention. Guidelines for prevention of nosocomial pneumonia. MMWR Morb Mortal Wkly Rep. 46: 1997; 1-79.
Prevention Measures • Proper hand washing, use of gloves, and measures to reduce contamination from respiratory therapy equipment • Universally recognized, often not performed, see observational study performed in an ICU setting 10% of health care workers washed their hands before having direct patient contact and only 32% washed their hands after patient contact • Risk factors for an outbreak of multi-drug-resistant Acinetobacter nosocomial pneumonia among intubated patients. Chest. 115: 1999; 1378-1382.
Reduction of HCAP Incidence • Reduce immunosuppression, reduce sedation, avoid transportation of patients out of the ICU, and provide adequate nutrition • Oral placement of endotracheal or gastric tubes (sinusitis reduction) • Subglottic secretion drainage, continuous suction of oropharyngeal secretions in an effort to prevent pooling and thus aspiration • Semirecumbent position prevents aspiration of refluxed gastric contents • Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: A randomised trial. Lancet. 354: 1999; 1851-1858.
Reduction of HCAP Incidence • Administration of prophylactic antibiotics or nonabsorbable antibiotics for the purpose of gastrointestinal decontamination • Not shown to influence mortality or length of stay, use of antibiotics in this manner may lead to the development of resistant organisms • International conference for the development of consensus on the diagnosis and treatment of ventilator-associated pneumonia. Chest. 120: 2001; 955-970. • Results regarding the role of histamine blockers in the development of HAP are conflicting • Antibiotics select out resistant or virulent organisms, 65% of PNA in vented patients who received prophylactic abx was caused by Acinetobacter and /or Pseudomonas sp. • In antibiotic-naïve patients, only 19% of infections were caused by these pathogens • Nosocomial pneumonia in patients receiving continuous mechanical ventilation. Prospective analysis of 52 episodes with use of a protected specimen brush and quantitative culture techniques. Am Rev Respir Dis. 139: 1989; 877-884.
Things to Remember • HACP, HAP, VAP = BAD for the patient • Quantitative diagnostic microbiology- controversial! • Cover likely bugs promptly • Know your local bugs • De-escalate, shorten duration of therapy • Specific regimen, combination therapy- no proven benefits
Things to Do • Get patient’s HOB at 30-45 degrees • Get the ET tube out • Get the NG tube out • Get of the ventilator as ap