Download
1 / 26
260 likes | 490 Views
Ethical Challenges in Clinical Testing of Microbicides. On-Going Discussion and Debate. Lori Heise Microbicides 2004. GCM Role in Ethics. GCM goals viz a viz ethics: Help give voice to community and civil society perspectives on trial design and ethics issues

E N D
Ethical Challenges in Clinical Testing of Microbicides On-Going Discussion and Debate Lori Heise Microbicides 2004
GCM Role in Ethics • GCM goals viz a viz ethics: • Help give voice to community and civil society perspectives on trial design and ethics issues • Help forge consensus around ethical debates that could delay progress • Negotiate difficult line between urgency of the HIV epidemic and maintaining rigorous ethical standards • Build capacity in the activist/community sector for ethical deliberation and debate
Microbicide Ethics Consultations Earliest ethics consultation initiated by advocates in 1997 – 55 participants from 23 countries Pre-dated launch of phase II or III studies of novel microbicides in developing countries Ethics working group of HPTN Global Campaign ethics consultations held in March and October of 2004
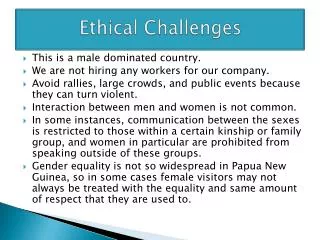
Special Challenges in Microbicide Trials • Complex clinical trial design • New, unfamiliar type of product • Healthy individuals -- yet at “high risk” • Results affected by user behavior • Sensitive issues – sex, power, gender • Stigma associated with HIV and sexual activity • Transnational collaborations
Family Planning Condom plus placebo INFORMED CONSENT to be SCREENED INFORMED CONSENT to be ENROLL Recruitment: Participant receives information about the trial. Screening Visit 1: Education about the trial, HIV and pregnancy test, STD tests and treatment, baseline data collected Screening Visit 2: Results of tests, counseling, reinforce education about trial Raqndomization: Participant assigned by chance to a group. Condom plus experimental gel Experience of a Phase 3 participant Condom only ????
Ethical Issues in Microbicide Trials • Equitable distribution of burdens and benefits -- Avoiding exploitation • Avoiding “wishful thinking” – also known as the“therapeutic misconception” • Standard of care for trial participants • What package of prevention and care should be provided to trial participants? • What obligation do we have to those who seroconvert during a trial?
Avoiding Exploitation • “Are trial participants guinea pigs?” • Based in historic experience of exploitation of vulnerable populations for research • Why are you doing the trial here? • Need to “unpack” the issues and implications around this statement.
Unpacking Concerns • Who is conducting the research? • Who benefits from the research? • Why do the research among this population/ community? • What will the research contribute? • Are trial participants “expendable?” • Who makes decisions about this research?
Why are most of the phase III trials taking place in Africa and Asia? • Microbicide trials require large numbers of women at risk of vaginally transmitted HIV • High incidence • Relatively stable (non-transient population) • Little or no injection drug use • Anal sex relatively uncommon • Most populations of women in the US or Europe with high HIV incidence also use IV drugs
Sample Size Calculations Effectiveness Annual HIV Sero-Incidence 1% 2% 3% 4% 5% 20% 110266 54638 36094 26824 21259 30% 46315 22965 15181 11289 8955 40% 24539 12176 8056 5995 4760 50% 14736 7320 4847 3609 2868 60% 9560 4753 3612 2351 1868 70% 6529 3249 2158 1612 1282 80% 4621 2304 1532 1144 913 90% 3353 1673 1115 835 666 Notes: Significance level = .05, power = 90%, test statistics and log rank test, two-tailed, equal size groups. Assumes 15 percent loss to follow-up. Figures prepared by Charlotte Ellertson and Kelly Blanchard using nQuery (version 1.0) survival analysis option.
clinical trial sites Antwerp, Belgium London, UK New York, USA Cincinnati, USA Washington, USA Providence, USA Philadelphia, USA Los Angeles, USA Baltimore, USA Norfolk, USA Houston, USA Ghana Birmingham, USA Côte d’Ivoire India Chiang Rai,Thailand Miami, USA Dominican Republic Nigeria Uganda Yaoundé, Cameroon Tanzania Malawi Zimbabwe Zambia Brazil Botswana South Africa Alliance for Microbicide Development
` Condoms + placebo gel Risk Condoms + microbicide (if it works) Before trial During Trial Will participating in trials increase women’s risk of HIV? • Generally, no... • Women will become infected during the trial but not because of the trial • Women in both arms should have lower HIV prevalence than women in the general community Condoms only Condom only
Therapeutic misconception • Therapeutic misconception” refers to the tendency of some research participants to wrongly assume that whatever drug or intervention they are offered must work or be beneficial (or why would it be offered?) • It occurs when the goals of research and those of therapy or “health care” become confused in the participants mind. • The therapeutic misconception is a major threat to “informed consent” in microbicide trials
“Standard of Care” • The term “Standard of care” refers to the nature of the prevention and/or care that will be provided to participants in research • It has been used variously to refer to: • the general care and treatment that investigators agree to provide all participants in clinical research • And more specifically to: • the quality of care that should be provided to people in the control arm of a RCT – i.e. those that are not receiving the experimental intervention
The Standard of Care Debate • The appropriate “Standard of Care” in international trials has been subject to intense debate • Heated up around controversial HIV trials to prevent mother to child transmission in the developing world • Commentators questioned the ethics of trials that used a “placebo” when an existing regimen 076 had been shown to reduce peri-natal transmission of HIV in the United States • Defenders argued that the 076 protocol was not “relevant” to the health care needs or priorities of the developing world, because it could not viably be implemented
SOC Debate as Applied to Microbicides • What package of prevention services should participants in the control arm of a trial be provided? • High standard HIV counseling, condoms, STD screening, treatment? Investigator’s Dilemma The more effective your prevention package is, the more difficult it becomes to determine whether the product works
Standard of Care (continued) • What other health care should be provided during the trial? • Pap tests? Family Planning? Malaria Rx? • What HIV care should individuals who seroconvert during the trial be provided? • TB prophylaxis, nutrition counseling, support groups, MTCT, ARVs? • What care, if any is due women who are screened out of the trial because they are already HIV+?
Issues raised • Is it ever ethical to provide different health packages in different settings? • Should we be more concerned about North/South inequities or exacerbating local inequities? • Is it possible to conduct ethical research in a fundamentally unjust world? • Whose voices should be part of the decision making process?
HIV Treatment in the context of prevention trials • Discourse has changed dramatically since 1997 – ART not even topic of discussion at the first microbicide ethics consultation • Long and complex discussion has taken place in the vaccine community – led by UNAIDS • In earlier UNAIDS regional consultations delegates were unable to reach consensus over whether vaccine trials should guarantee access to ART • Drop in drug prices has re-kindled debate and brought ART within grasp of the developing world
Divergent Regional ConclusionsUNAIDS Vaccine consultations 1998-2001 • Brazil: At the level of the sponsor country and should include ART at least for the duration of the trial and longer, if so negotiated • Thailand: At a level decided upon by the host country, including monitoring, prevention and treatment of opportunistic infections and palliative care, but not necessarily including ART, but what ever provided should be made reasonably available for the lifetime of the participants • Uganda: At the level consistent with that available in the host country; there is no imperative to provide a level of care consistent with that in the sponsoring country or with the highest available in the world.
Competing considerations • Belief that sponsors have an ethical obligation to provide care and treatment according to their resources • A desire to achieve equity in care and treatment received by participants in sponsor and host countries • Belief that participants deserve the best available care in light of the risks they have assumed for the larger good • Concern by some that promising ART to trial participants might create “undue inducement” to participate if drugs are otherwise unavailable locally • Concern that providing ART only to trial participants might exacerbate local inequities and create problems within families and communities VS.
Competing Considerations (continued) • The notion that sovereign nations and communities have the right to determine for themselves the balance of risks and benefits they are willing to accept • Concern that governments might abdicate on their responsibility to provide care and treatment if sponsors fill this role • The belief that host communities themselves should have a say in helping decide the package of care and services that maximize the benefit of the trial to participants and the community • Desire to ensure that poorer countries could continue to attract research to their countries in order to address the critical need of their populations for an HIV vaccine
Discussion in Microbicide World • Enormous commitment to improving local standard of care, including HIV care • Less clarity that ART should be guaranteed in all cases – concern to also emphasize other aspects of care • Trial sponsors are actively debating their policies, and exploring mechanisms for providing care • Interest in getting more input from the host communities on their opinions • Concern about local inequities created, including what to do with hundreds of HIV positive women screened out of trials • Recognition that what vaccine community does may create precedent for other prevention trials
Emerging consensus among vaccine trial sponsors • Participants who seroconvert during a trial should be provided treatment, including ART • Still disagreement about whether this is an ethical minimum/ obligation, or a morally praiseworthy act • Continued debate about whose obligation it is to provide this treatment – the trial sponsors, host country governments, sponsoring nations? • Clear commitment to try to leverage outside resources to maximize likelihood that ART will be made available in trial communities • Focus to date has been on treatment of those who seroconvert, not those screened out, partners of family members.
The debate continues… • Is access to ART the best way to maximize justice and social good in microbicide trials? • Is it fair for participants to get ART, but those who are screened out get nothing? • Would it be better to provide less high tech care to more people? • Is the sustainability of an interventional morally relevant? • Who should decide?
Moving the debate from Geneva to Capetown • Ethics is a process of moral reflection, not a set of rules • How decisions are arrived at is ethically relevant • Whose voice is represented in the debate is therefore important • Advocates and communities must prepare themselves to become active participants in these debates GCM Course in Ethical Reasoning