Download
1 / 51
580 likes | 927 Views
Robotic Surgery in Urology Dr. Wong Wai Sang FRCS, FRACS, FHKAM, FRACS(Urology). Urological Surgery in The Last Century Open surgery – 100 years. Urological Surgery in The Last Century Open surgery – 100 years. Urological Surgery in The Last Century Open surgery – 100 years.

E N D
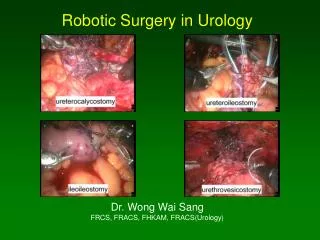
Robotic Surgery in UrologyDr. Wong Wai SangFRCS, FRACS, FHKAM, FRACS(Urology)
Urological Surgery in The Last CenturyOpen surgery – 100 years
Urological Surgery in The Last CenturyOpen surgery – 100 years
Urological Surgery in The Last CenturyOpen surgery – 100 years
Urological Surgery in The Last CenturyOpen surgery – 100 years
Urological Surgery in The Last CenturyLaparoscopic surgery – 10 yearsUrological Surgery at The Turn of The CenturyRobotic Surgery
Minimally Invasive SurgeryLaparoscopic Surgery • Muhe performed the first laparoscopic cholecystectomy in 1985 but rejected by the German Surgical Society • Mouret performed the first laparoscopic cholecystectomy in 1987 • Perissat demonstrated the technique of laparoscopic cholecystectomy at the Society of American Gastrointestinal Surgeons Meeting in Louisville in 1989 • Spread rapidly all over the world • First laparoscopic cholecystectomy done in HK in 1990
Laparoscopic SurgeryAdvantages • Decreased pain • Shorter hospital stay • Rapid return to work • Smaller scars • Less infection • Less bleeding
Laparoscopic Radical Prostatectomy • Schuessler (1997) – had no advantages over open surgery because of the difficulties and long hours of the operation • Vallancien (1999), Abbou (2000) – laparoscopic radical prostatectmy was feasible • Ahlering (2003) – learning curve for laparoscopically naïve surgeon was 80-100 cases, learning curve for skilled laparoscopic surgeon was 40-60 cases (median number of radical prostatectomy performed by US urologists was 7 per year)
Laparoscopic SurgeryDisadvantagesdecreased surgeon’s dexterity, control, precisionmore surgeon’s fatigue and tirednessvery difficult in operating complex surgery
Means to Overcome Decrease Dexterity • Clip • Haemolock • Stapler • Endoloop • Extracorporeal knot tying • Ligasure • Harmonic scalpel • Argon beam coagulator To escape from the difficulties in suturing and knots tying
Robotic Surgical Systems • To overcome the problems from complex surgery meticulous dissection suturing knots tying
Da Vinci Surgical SystemSurgical robot • Robot – a mechanical device incorporated with a computer • Master-slave system – the surgeon directly initiates all the movements of the robotic instruments in real time • Robotic radical prostatectomy – robotic assisted laparoscopic radical prostatectomy retain the advantages of minimally invasive surgery overcome the drawbacks of conventional laparoscopic surgery
Da Vinci Surgical System • The prototype was developed by Stanford Research Institute in 1980s, funded by US Army, to perform battlefield surgery remotely by a surgeon in the safe rear • FDA approved in human operations in 2000 • “Targeted at the heart, but hit the prostate” • By the end of 2006, 559 robots have been installed worldwide, 392 robots were in US • In 2006, over 70,000 robotic surgery were performed Over 30,000 robotic surgery were for prostate cancer • In US, <1% of the radical prostatectomy were done by robots in 2001, >40% of the radical prostatectomy were done by robots in 2006
Da Vinci Surgical SystemHuman eye vision and beyond • Double lenses laparoscope • 3D, high definition, binocular view • 10-15X magnification
Da Vinci Surgical SystemHuman hand dexterity and beyond • Endowrist instruments have 6 degrees of freedom • Filtering off hand tremor • Scaling down movements 1-5X
Da Vinci Surgical System • Improved dexterity • Better control • Better precision • Improved ergonomics – decreased fatigue and strain
Da Vinci Surgical SystemShort learning curve & better results • Ahlering - surgeons with experience in open techniques but no laparoscopic experience, the results of after performing 8 - 12 robotic radical prostatectomy were comparable to those of skilled laparoscopists who had performed more than 100 laparoscopic radical prostatectomy T Ahlering J Urol 2003 • Robotic radical prostatectomy vs open radical prostatectomy Improved cancer control Increased continence Enhanced sexual potency V Patel J Endourol 2005 T Ahlering ART 2006 M Menom UCNA 2004
Experience of robotic radical prostatectomy from different centers in the world patients OT blood loss hospital stay catheter +ve margin Binder 10 450 mins - - 18 days 30% Rassweiler 6 315 mins - - 7.3 days 0% Bentas 40 8.3 hrs 570 ml - - - Ahlering 60 231 mins 103 ml 25.9 hrs 7 days 16.7% Menon 40 274 mins 256 ml - - 18% Menon 200 160 mins 153 ml 1.2 day 7 days 6%
Operative parameters for conventional, laparoscopic & robotic radical prostatectomy OT blood loss catheter complications +ve margin (min) (ml) (day) (%) (%) RRP Lepor 131 820 7-14 6.6 17 Catalona 217 1395 7-14 10 21 LRP Montsouris 217 345 6.6 13.3 17 Abbou 271 NA 9 11.7 18.1 RAP Menon 160 153 7 5 6
Odd ratio for important outcomes for laparoscopic, robotic & radical retropubic prostatectomy performed at the Vattikuti Urology Institute Variable open laparoscopic robotic (reference value) (odd ratio) (odd ratio) Operating time 163 mins 1.51 0.91 Blood loss 910 ml 0.42 0.10 Positive margin 23% 1 1 Complication 15% 0.67 0.33 Catheter time 15.8 days 0.5 0.44 Hospital >24 hours 100% 0.35 0.07 Postop pain score 7 0.45 0.45 (0-10) Mean time to continence 160 days 1 0.28 Mean time to erection 440 days NA 0.4 Mean time to intercourse >700 days NA 0.5 Detectable PSA 15% 1 0.5 M Menom UCNA 2004
Urology radical prostatectomy 17 radical cystectomy 3 partial nephrectomy 3 ureterocalycostomy 2 pyeloplasty 1 ureteroureterostomy 1 Lower GI APR 1 Gynecology hysterectomy 2 Paediatric Surgery reimplantation of ureter 8 pyeloplasty 6 excision of ureterocele 2 Upper GI wedge excision of stomach 3 fundoplication 1 Heller cardiomyotomy 1 Cardiothoracic Surgery thymectomy 1 Robotic SurgeryPWH(Nov 2005 – Nov 2006)
Da Vinci S Surgical System • Fast foolproof setup • Rapid instrument exchange • Multi-quadrant access • Interactive video display
Robotic SurgeryHKSHMarch 2007 – July 2007 • Radical prostatectomy 29 • Partial nephrectomy 2 • Pyeloplasty 1 • Hysterectomy 2 • Tubal reanastomosis 2