Pleurisy
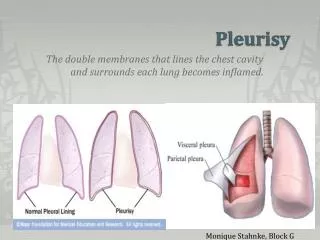
Pleurisy. Andriy Lepyavko, MD, PhD Department of Internal Medicine № 2. Pleurisy is inflammation of the pleura. . Classification: Dry pleurisy (pleuritis sicca) Pleurisy with effusion (pleuritis exudativa)

Pleurisy
E N D
Presentation Transcript
Pleurisy Andriy Lepyavko, MD, PhD Department of Internal Medicine № 2
Pleurisy is inflammation of the pleura. Classification: Dry pleurisy (pleuritis sicca) Pleurisy with effusion (pleuritis exudativa) The character of the inflammatory effusion may be different: serous, serofibrinous, purulent, and haemorrhagic.
Etiology and pathogenesis • Serous and serofibrinous pleurisy (tuberculosis in 70-90 per cent of cases, pneumonia, certain infections, and also rheumatism in 10-30 per cent of cases) • Purulent process (pneumococci, streptococci, staphylococci, and other microbes) • Haemorrhagic pleurisy (tuberculosis of the pleura, bronchogenic cancer of the lung with involvement of the pleura, and also in injuries to the chest)
DRY PLEURISY Clinical picture • pain in the chest (a characteristic symptom )which becomes stronger during breathing and coughing. • cough (is usually dry) • general indisposition; • subfebrile temperature • Respiration is superficial (deep breathing intensifies friction of the pleural membranes to cause pain). Lying on the affected side lessens the pain. Inspection of the patient can reveal unilateral thoracic lagging during respiration. Percussion fails to detect any changes except decreased mobility of the lung border on the affected side. Auscultation determines pleural friction sound over the inflamed site.
Normal pleural fluid has the following characteristics: clear ultrafiltrate of plasma, pH 7.60-7.64, protein content less than 2% (1-2 g/dL), fewer than 1000 WBCs per cubic millimeter, glucose content similar to that of plasma, lactate dehydrogenase (LDH) level less than 50% of plasma and sodium, and potassium and calcium concentration similar to that of the interstitial fluid.
Transudative pleural effusion • Congestive heart failure (most common transudative effusion) Hepatic cirrhosis with and without ascitesNephrotic syndrome Peritoneal dialysis/continuous ambulatory peritoneal dialysis Hypoproteinemia (eg, severe starvation) GlomerulonephritisSuperior vena cava obstruction Urinothorax
Exudative pleural effusion • Malignant disorders - Metastatic disease to the pleura or lungs, primary lung cancer, mesothelioma, Kaposi sarcoma, lymphoma, leukemia • Infectious diseases - Bacterial, fungal, parasitic, and viral infections; infection with atypical organisms such as Mycoplasma, Rickettsiae, Chlamydia, Legionella • GI diseases and conditions - Pancreatic disease (acute or chronic disease, pseudocyst, pancreatic abscess), Whipple disease, intraabdominal abscess (eg, subphrenic, intrasplenic, intrahepatic), esophageal perforation (spontaneous/iatrogenic), abdominal surgery, diaphragmatic hernia, endoscopic variceal sclerotherapy • Collagen vascular diseases - Rheumatoid arthritis, systemic lupus erythematosus, drug-induced lupus syndrome (procainamide, hydralazine, quinidine, isoniazid, phenytoin, tetracycline, penicillin, chlorpromazine), immunoblastic lymphadenopathy (angioimmunoblastic lymphadenopathy), Sjцgren syndrome, familial Mediterranean fever, Churg-Strauss syndrome, Wegener granulomatosis
Benign asbestos effusion • Meigs syndrome - Benign solid ovarian neoplasm associated with ascites and pleural effusion • Drug-induced primary pleural disease - Nitrofurantoin, dantrolene, methysergide, bromocriptine, amiodarone, procarbazine, methotrexate, ergonovine, ergotamine, oxprenolol, maleate, practolol, minoxidil, bleomycin, interleukin-2, propylthiouracil, isotretinoin, metronidazole, mitomycin • Injury after cardiac surgery (Dressler syndrome) - Injury reported after cardiac surgery, pacemaker implantation, myocardial infarction, blunt chest trauma, angioplasty • Uremic pleuritis • Yellow nail syndrome • Ruptured ectopic pregnancy • Electrical burns
PLEURISY WITH EFFUSION Clinical picture • Complains: fever, pain or the feeling of heaviness in the side, dyspnea (which develops due to respiratory insufficiency caused by compression of the lung). Cough is usually mild (or absent in some cases). • Objective examination: The patient's general condition is grave, especially in purulent pleurisy, which is attended by high temperature with pronounced circadian fluctuations, chills, and signs of general toxicosis. Inspection of the patient reveals asymmetry of the chest due to enlargement of the side where the effusion accumulated; the affected side of the chest usually lags behind respiratory movements. Vocal fremitus is not transmitted at the area fluid accumulation.
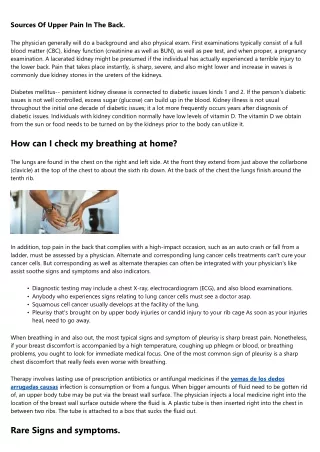
Cyanosis in pleurisy with effusion due to respiratory insufficiency is caused by lung collapse and limitation of its respiratory surface
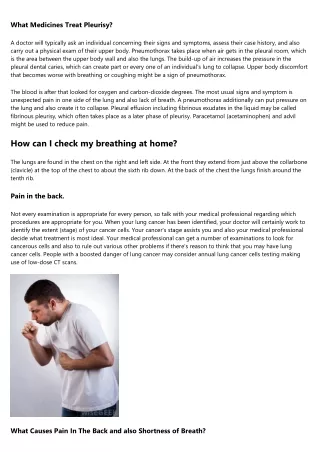
Percussion over the area of fluid accumulation produces dullness. The upper limit of dullness is usually the S-shaped curve (Damoiseau's curve) whose upper point is in the posterior axillary line. The effusion thus occupies the area, which is a triangle both anteriorly am posteriorly. The Damoiseau curve is formed because exudate pleurisy with effusion more freely accumulates in the lateral portions of the pleural cavity, mostly in the costal-diaphragmatic sinus.
In addition to the Damoiseau curve, two triangles can be determined by percussion in pleurisy with effusion. The Garland triangle is found on the affected side is characterized by a dulled tympanic sound. It corresponds to the lung pressed by the effusion, and is located between the spine and the Damoiseau curve. The Rauchfuss-Grocco triangle is found on the healthy and is a kind of extension of dullness determined on the affected side, sides of the triangle are formed by the diaphragm and the spine, while the continued Damoiseau curve is the hypotenuse.
Pleurisy with effusion: posterior view: 1—Damoiseau's curve;2—Garland's triangle; 3—Rauchfuss-Grocco triangle.
Treatment • Antibiotics (eg, for parapneumonic effusions) and diuretics (eg, for effusions associated with CHF) are commonly used in the initial management of pleural effusions in the ED. The selection of drugs in each class depends on the cause of the effusion and its clinical presentation. Particular attention must be given to potential drug interactions, adverse effects, and preexisting conditions.
Tuberculous pleural effusion • TB remains the most common cause of pleural effusion in young people • Etiology: tubercle bacillus • Pathogenesis: host hypersensitivity to tubercular protein in pleural tubercles • Delayed hypersensitivity
Clinical Manifestations • Generalized symptoms of toxicity of TB: fever, sweats, fatigue, weight loss ss, etc. • Pleuritic pain, dyspnea, coughlea, etc. • Pleural fluid is exudative and usually reveals lymphocytosis • Rarely pleural fluid is blood stained • Tubercular tests usually positive
Empyema • Thick purulent fluid with more than 100,000 cells per cubic millimeter or fluid with PH values less than or equal to 7. 20 should be treated as a presumptive empyema • The general objectives of therapy of empyema are the elimination of both the systemic and local infection.
Treatment of acute and chronic empyema 1. Control of infection systemic and local 2. Repeated thoracentesis or drainage of the empyema 3. Chronic empyema is primarily treated operatively 4. Operative therapy is also indicated in the empyema with associated bronchopleural fistula or with the ipsilateral ruined lung